William D. Anderson, III, MD, DABFM, FAAFP Nathaniel S. Treister, DMD, DMSc E.J. Mayeaux, Jr., MD, DABFM, FAAFP Romesh P. Nalliah, DMD University of South Carolina School of Medicine, Columbia (Drs. Anderson and Mayeaux); Brigham and Women’s Hospital, Boston (Dr. Treister); Harvard Medical School, Boston (Dr. Nalliah) william.anderson@uscmed.sc.edu
The authors reported no potential conflict of interest relevant to this article.
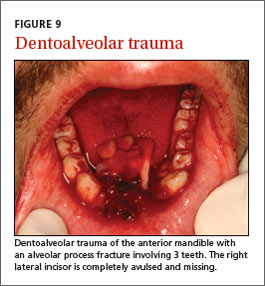
Trauma. Dental trauma can be limited to the teeth and soft tissues, while more severe injuries can also affect the jaw bone.9 Accidental falls, assault, and motor vehicle traffic accidents are the most common causes of facial fractures in the United States, and are often associated with dentoalveolar trauma (FIGURE 9). The most commonly fractured facial bone is the mandible, characterized by painful opening and closing and an incomplete or altered bite.10
Oral symptoms may be the first sign of systemic disease
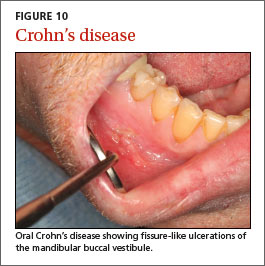
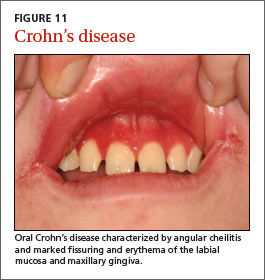
Inflammatory bowel disease. Crohn’s disease may affect the gastrointestinal tract anywhere from the mouth to the anus and may initially present with oral findings that may not correlate with abdominal symptoms. Oral Crohn’s disease may present as mucosal cobblestoning, mucosal tags, deep linear ulcerations, gingival hyperplasia, lip fissuring, aphthous ulcers, and angular cheilitis (FIGURES 10 AND 11). Other features may include diffuse, painless swelling of the lips and mucosal erythema.
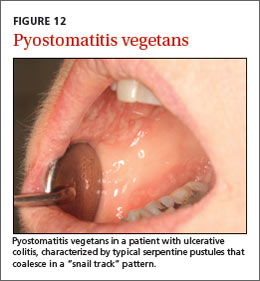
Pyostomatitis vegetans is an uncommon condition typically associated with ulcerative colitis that is characterized by serpentine pustules that coalesce in a “snail track” pattern (FIGURE 12).11
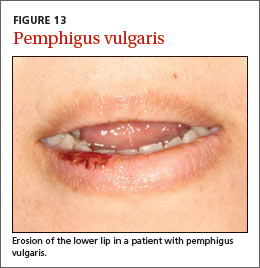
Dermatologic/vesiculo-bullous diseases. Vesiculo-bullous lesions in the mouth may be seen in pemphigus vulgaris or bullous pemphigoid. Pemphigus vulgaris is an autoimmune intraepithelial blistering disease that often first presents in the oral cavity as flaccid bullae or painful ulcerations, prior to the onset of skin lesions (FIGURE 13).
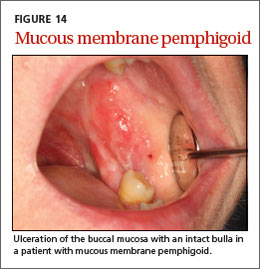
Mucous membrane pemphigoid is an autoimmune subepithelial disease that affects mucous membranes and the skin. Characteristic oral mucosal blisters quickly rupture and form ulcerations, which may be present in the absence of other mucosal involvement (eg, anus, genitalia, nose or throat) (FIGURE 14).12 Painful aphthous ulcers are common. When oral ulcerations are diffuse and recurrent, they may be the first sign of Behçet’s disease, a multisystem autoimmune vasculitis.13
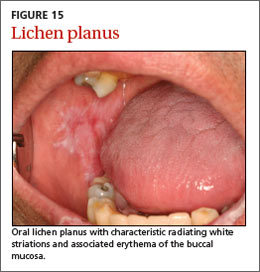
Oral lichen planus is a chronic immunemediated mucocutaneous disease that is often limited to the oral cavity. It presents with characteristic radiating white striations of the buccal mucosa and tongue, often with associated erythema and ulcerations (FIGURE 15).14
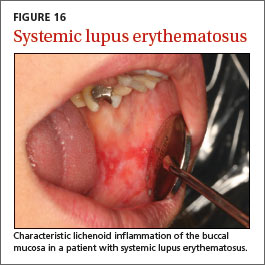
Rheumatologic conditions. Systemic or discoid lupus erythematosus may present with oral findings that largely resemble those of oral lichen planus (FIGURE 16).15 Sjögren’s syndrome is an autoimmune disease with characteristic xerostomia, which can lead to oral discomfort, dysphagia, recurrent candidiasis, and rampant dental caries.
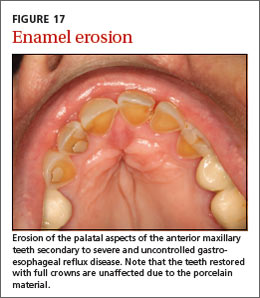
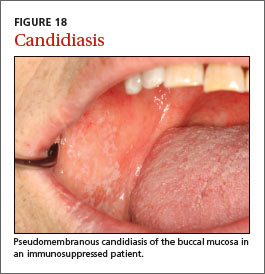
Other conditions to watch for. Erosion of the enamel on the lingual surface of the teeth may be a sign of gastroesophageal reflux disease or bulimia (FIGURE 17). Examination of the oral mucosa can reveal typical white plaques of oral candidiasis (FIGURE 18), which may be associated with systemic immune suppression as well as salivary gland dysfunction.
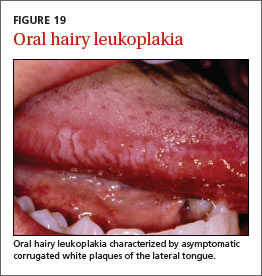
Oral conditions that have been associated with human immunodeficiency virus infection include ANUG/ANUP, recurrent candidiasis, and oral hairy leukoplakia (FIGURE 19). In the absence of known HIV infection, patients who present with any of these oral conditions should be evaluated for HIV infection.13 (For more on recognizing the signs of HIV infection in patients without classic risk factors, see “HIV: 3 cases that hid in plain site” [J Fam Pract. 2015;64:20-26]).
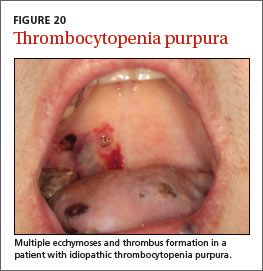
Atrophic glossitis may indicate a vitamin B deficiency. Thrombocytopenia and leukemia may present with oral petechiae, purpura, oral hematomas, or hemorrhagic bullae (FIGURE 20).13 Painless pseudomembranous mucosal erosions may be a presentation for secondary syphilis.16
Look for signs that suggest malignancy
In the United States, oral and pharyngeal cancers account for approximately 40,000 cases of cancer and 8000 deaths each year.17 More than 90% of these are squamous cell carcinomas (SCCs); the remainder are mainly salivary gland tumors, lymphoma, and other infrequent cancers.18
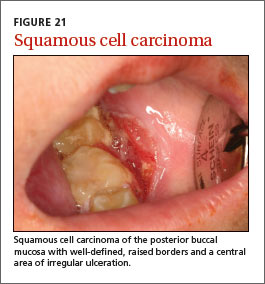
SCC of the oral cavity most commonly occurs on the tongue but can develop in any site, presenting as mucosal ulcers, plaques, or masses that do not heal (FIGURE 21). Tobacco and alcohol use are associated with up to 80% of cases of SCC of the head and neck.18 Some oropharyngeal SCCs are associated with human papillomavirus infection type 16.19
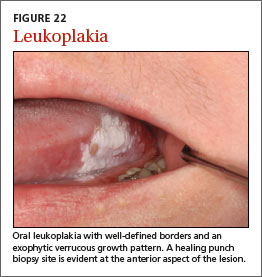
Potentially malignant oral lesions include leukoplakia and erythroplakia. Leukoplakia is a white patch or plaque of the oral mucosa that can’t be explained by any other clinical diagnosis (FIGURE 22). These lesions are at risk for malignant transformation and may demonstrate dysplasia or frank SCC on biopsy.20 Proliferative verrucous leukoplakia is a unique form of leukoplakia that’s characterized by a wrinkled appearance that is often multifocal; the condition is associated with a higher risk of malignant transformation.
Erythroplakia is a red patch that similarly can’t be explained by another diagnosis. It has a very high risk of malignant transformation over time. All potentially malignant oral lesions, including leukoplakia and erythroplakia, require biopsy and careful monitoring.