DENVER – Twice-daily treatment with the long-acting muscarinic antagonist glycopyrronium improved lung function and health status in patients with chronic obstructive pulmonary disorder (COPD) and moderate to severe airflow limitation in the randomized, double-blind, placebo-controlled GEM2 study.
In patients with stable symptomatic COPD with moderate to severe airflow limitation, twice-daily 12.5-mcg dosing of glycopyrronium provides clinically meaningful improvement in lung function over the 12-hour dosing interval, has early onset, is sustained over 12 weeks when compared with placebo, and is associated with significant improvements in COPD symptoms, health status, and rescue medication use, as well as numerical improvement in dyspnea scores, Dr. Edward Kerwin of the Clinical Research Institute of Southern Oregon, PC, Medford, and his colleagues reported in a poster at an international conference of the American Thoracic Society.
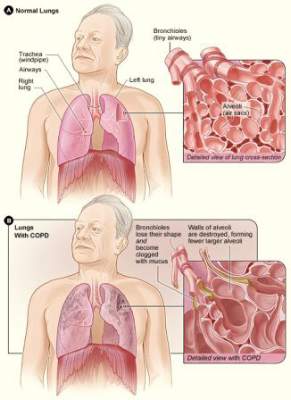 Courtesy NHLBI/National Institutes of Health
Courtesy NHLBI/National Institutes of Health
Lung function – as measured by forced expiratory volume in 1 second (FEV1) area under the curve from 0-12 hours (AUC 0-12h) – was significantly better both at day 1 and at week 12 of treatment in 216 patients who were randomized to receive a 12.5 mcg twice daily dose of the fast-onset, long-acting muscarinic antagonist (Novartis), compared with 216 patients who received placebo; there was a “significant and clinically meaningful between-treatment difference of 119 and 123 mL, respectively,” the researchers wrote.
“Glycopyrronium also showed consistently significant improvements in trough FEV1 vs. placebo at all assessed time points,” they said, adding that glycopyrronium showed an early onset of bronchodilation with significant improvements in FEV1 at 5 and 15 minutes post dose, compared with placebo at day 1 and week 12.
The least squares mean treatment differences for glycopyrronium vs. placebo for change from baseline in trough forced vital capacity (FVC) were 171 mL on day 2, and 130 mL at week 12. Peak FEV1 and peak FVC were significantly improved with glycopyrronium vs. placebo on day 1 (least squares mean treatment differences of 137 and 223 mL, respectively) and at week 12 (least squares mean treatment differences of 148 and 201 mL, respectively).
Health status was improved at week 12, with both significant and clinically meaningful improvements in St. George’s Respiratory Questionnaire total score in the treatment vs. placebo group (–6.4 vs. –1.2), and the percentage of patients achieving minimal clinically important differences (MCID), defined as at least 4 units, was significantly higher in the treatment vs. placebo group (54.9% vs. 42.3%), the investigators said.
Additionally, numerical improvements in transition dyspnea index total score, and percentage of patients achieving a MCID, defined as at least 1 unit, were observed at week 12 in the glycopyrronium vs. placebo group.
Patients in the glycopyrronium group showed improvement on all symptoms scores and endpoints, according to data recorded in patient e-diaries, and those in the treatment group also were able to perform usual daily activities significantly more often than those in the placebo group.
“A statistically significant decrease in daily, daytime, and nighttime number of puffs, and a significant increase in the percentage of days with no rescue medication use were observed,” the investigators noted.
Patients included in the multicenter GEM2 (Glycopyrronium Effect on Symptoms and Lung Function) study were adults aged 40 years and older with moderate to severe airflow limitation (GOLD 2011 strategy level 2 or 3), who were either current or former smokers with a smoking history of at least 10 pack-years. All had postbronchodilator FEV1 of at least 30% and less than 80% of the predicted value, and postbronchodilator FEV1/forced vital capacity ratio of less than 0.70 at a run-in visit. They also all had a modified Medical Research Council grade of 2 or greater at the run-in visit. Patients with a history of asthma or with a COPD exacerbation requiring treatment with antibiotics and/or systemic corticosteroids, and/or with hospitalization within 6 weeks of the screening and run-in periods were excluded, as were those with a history of long QT syndrome or whose corrected QT was greater than 450 ms at the run-in visit.
All underwent an initial 1- to 7-day washout period and a 2-week run-in period prior to randomization, as well as a safety follow-up period. Patients received either glycopyrronium 12. 5 mcg or placebo twice daily delivered via the Neohaler device for 12 weeks.
Treatment was generally well tolerated; of the 430 patients included in the safety set, 44 permanently discontinued treatment due to adverse events (4.6% and 4.2% in the treatment and placebo groups, respectively). The number who experienced at least one adverse event during the treatment period was similar in the two groups; COPD was the most common adverse event, occurring in 20.8% of those in the treatment group and 21.5% in the placebo group.