THE CASE
An 80-year-old man sought medical advice over the phone because he’d had sharp anal pain for 4 days. The pain increased during sitting and defecation. He was told he most likely had an acute anal fissure and was instructed to treat it with sitz baths, a stool-bulking agent, and a topical anesthetic. Despite these treatments, he continued to have intense anal pain.
Two days later, he presented to our practice complaining of severe anal discomfort and perianal swelling that made it almost impossible to sit. The patient led an active lifestyle and was otherwise healthy. He did not recall any injury to the perianal area.
THE DIAGNOSIS
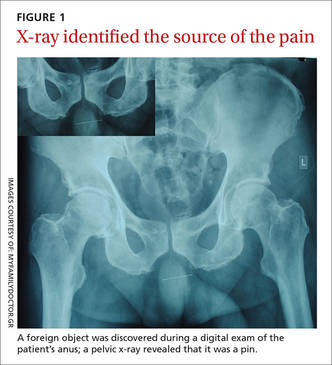
During examination, we noted tender, erythematous swelling over the right perianal region at the 9 o’clock position without fluctuance, discharge, or ulceration. A digital rectal examination revealed a foreign body lying transversely across the anus about 2.5 cm from the anal verge. A pelvic x-ray confirmed the presence of a foreign body—a pin (FIGURE 1).
DISCUSSION
Anal pain is a common symptom that is usually caused by hemorrhoids, fissures, fistulas, or abscesses.1 Anal pain is rarely reported to be secondary to the ingestion of sharp foreign bodies, which can produce problems in the lower gastrointestinal tract.
Foreign body ingestion is most common in children ages 6 months to 6 years.2 When it occurs in adults, it tends to involve those who are older, patients without teeth, prisoners, patients under the influence of drugs or alcohol, or those with intellectual disabilities or psychiatric disorders.2,3
The foreign bodies that adults most commonly unintentionally ingest are bones from fish or other animals.2,4 Most of these pass through the alimentary tract uneventfully within a week.2,5,6 Swallowed bones have been known to cause perianal abscesses and anal fistulae, which can cause extreme pain.7
The presence of foreign bodies is not always easy to spot
In our patient’s case, the diagnosis was made by a careful digital rectal examination; however, a foreign body in an abscess cavity can be missed during a digital exam.8 In our patient’s case, a pelvic x-ray confirmed the presence and location of the pin.
Radiography is recommended as an initial screening method and is especially useful for determining the location of radiodense foreign bodies.2 However, most swallowed foreign bodies, such as non-radiodense fish bones, wood, thorns, plastic, small aluminum objects, and glass, cannot be detected by this method.3 Non-radiodense foreign bodies can be identified using computed tomography scanning.9
Removal is typically straightforward
The best method of removing a foreign body in the perianal region is by dilating the anus and then cutting the object in half. Alternatively, the object can be carefully dislodged from the anal canal by freeing one of the impacted ends. Care must be taken while removing the object to avoid accidental injury.
This procedure can be performed in any primary care setting that is adequately equipped for minor surgical services. Consider referral to a secondary care specialist based on the level of risk involved and the physician’s skills and training.
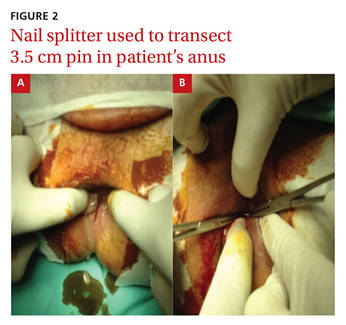
Our patient. After a complete assessment, we prepared the patient for gentle anal dilatation under intravenous conscious sedation. We carefully transected the 3.5 cm pin using a nail splitter (FIGURE 2). Because there was no abscess cavity, no other procedure was needed. We prescribed oral amoxicillin/clavulanic acid 500/125 mg every 8 hours for 7 days to treat a local infection.
After the procedure, we asked the patient about the pin. He said he had no idea how he could have ingested it and didn’t recall any abdominal pain during the previous month. Follow-up was normal, and he recovered without any complications.
THE TAKEAWAY
Consider the possibility of ingested sharp foreign bodies as a cause of severe anal pain, and perform a local and digital rectal examination. Radiography is recommended as an initial screening method. Following anal dilatation, the object can be removed by cutting it in half or by freeing one of the impacted ends.