Michael E. Cobble, MD, AAFP, FNLA Director, Canyons Medical Center, Adjunct Faculty, University of Utah School of Medicine, Sandy, UT, Chief Medical Officer, Atherotech, Birmingham, AL
Dr. Cobble has disclosed that he is on the advisory boards and speakers’ bureaus for AstraZeneca and Bristol-Myers Squibb and is on the speakers’ bureaus for Eli Lilly, Forest, and Kowa.
SUPPORT
This program is sponsored by the PCEC and is supported by funding from AstraZeneca.
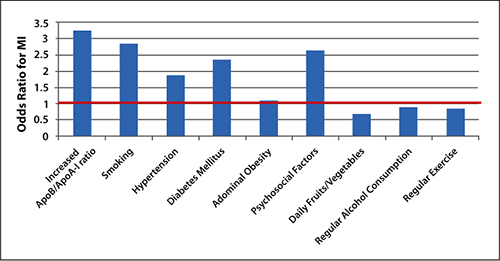
The death rate from coronary heart disease (CHD) declined by 59% from 1950 to 1999 in the United States, yet CHD remains a major cause of morbidity and mortality, resulting in an estimated 1.5 million heart attacks in 2011.1 Better recognition and treatment of the 9 modifiable risk factors for CHD identified by the INTERHEART study (FIGURE 1), as well as changes in lifestyle practices, undoubtedly contributed to the decline in CHD mortality, but further improvement is possible.2 Estimates derived from the Second National Health and Nutrition Examination Survey (NHANES II) baseline data and 17-year mortality follow-up data indicate that 45% of CHD deaths in men and 64% in women could be avoided by eliminating 3 major risk factors: elevated total cholesterol (≥240 mg/dL), hypertension, and smoking.3
The evidence indicates that these 3 risk factors are not well controlled. Data from the National Cholesterol Education Program (NCEP) Evaluation ProjecT Utilizing Novel E-Technology (NEPTUNE) II survey and the Lipid Treatment Assessment Project 2 (L-TAP 2), as well as more recent evidence, indicate that many patients do not achieve low-density lipoprotein cholesterol (LDL-C) and triglyceride targets.4-10 Similarly, although there has been significant improvement in blood pressure (BP) control over the past 2 decades, BP is controlled in only half of all hypertensive patients.11,12 Finally, the sharp declines in the prevalence of cigarette smoking seen in the past have slowed in recent years, such that approximately 20% of US adults still smoke cigarettes.13
These trends are a concern since a greater risk factor burden in middle age is associated with poorer quality of life and higher medical costs, as well as a higher incidence of cardiovascular events in older age.1 A recent meta-analysis of 18 cohort studies involving 257,384 adults showed a higher incidence of cardiovascular events in later life with an increasing number of risk factors.14 For example, adults 55 years of age with an optimal risk factor profile (ie, total cholesterol <180 mg/dL, BP <120/80 mm Hg, nonsmoker, nondiabetic) had much lower risks of death from cardiovascular disease (CVD) through the age of 80 years than those with 2 or more risk factors (4.7% vs 29.6% among men, 6.4% vs 20.5% among women). This translates into a relative risk (RR) of cardiovascular death of 6 times for men and 3 times for women without optimal risk profiles. Similar trends were observed for risk of fatal CHD/nonfatal myocardial infarction (MI) (3.6% vs 37.5% among men, <1% vs 18.3% among women). These findings point to the critical importance of modifying multiple risk factors early in adulthood, well in advance of symptoms. However, the Study to Help Improve Early Evaluation and Management of Risk Factors Leading to Diabetes (SHIELD) showed that about half of patients with CHD are not diagnosed until symptoms become apparent, and fewer than one quarter are diagnosed as a result of screening.15
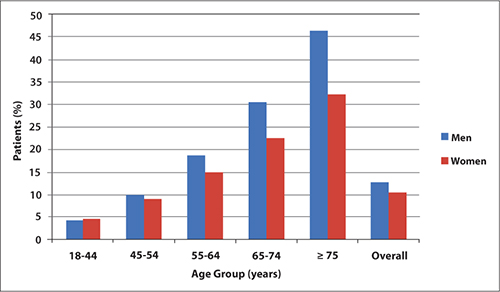
This review focuses on patient assessment and treatment strategies to modify abnormal lipid levels and high BP for primary prevention. Addressing other modifiable risk factors is also important, especially since risk factors such as abdominal obesity impact other risk factors (FIGURE 1). An emphasis is placed on strategies in men, since the prevalence of CHD among patients aged 45 years and older is higher in men than in women (FIGURE 2).16 Furthermore, men experience a first cardiovascular event a decade earlier than women, and a more serious CHD event, such as MI or sudden death, 2 decades earlier.1
FIGURE 1
Modifiable risk factors for myocardial infarction (MI)2
The assessment of CHD risk in men need not be complicated and should be made practical so that it is applied consistently. A family and personal medical history and physical examination combined with laboratory determination of lipid levels and glycosylated hemoglobin can help assess modifiable risk factors. The assessment of CHD risk can be facilitated by using 1 of 2 risk calculators. The Framingham Risk Score [www.framinghamheartstudy.org/risk/gencardio.html] is widely used but may underestimate risk, especially in younger persons or those who appear to be healthy but may have other risk factors for CHD.17-19 The Reynolds Risk Score [www.reynoldsriskscore.org/] includes other risk factors, such as parental history of MI before age 60 years, low levels of apolipoprotein A (apoA), high levels of apolipoprotein B (apoB), and increased levels of high-sensitivity C-reactive protein (hs-CRP).19 The Reynolds Risk Score has been validated in healthy, nondiabetic men.20