TABLE 2
Antihypertensive treatment in patients with compelling indications41,49
| Indication | Diuretic | BB | ACEI | ARB | Calcium antagonist | Aldosterone antagonist |
|---|---|---|---|---|---|---|
| Heart failure | ||||||
| Post MI | ||||||
| CVD or high CVD risk | ||||||
| Anginaa | ||||||
| Aortopathy/aortic aneurysma | ||||||
| Diabetes | ||||||
| Recurrent stroke prevention | ||||||
| CKDb | ||||||
| Early dementiaa | ||||||
ACCF, American College of Cardiology Foundation; ACEI, angiotensin-converting enzyme inhibitor; AHA, American Heart Association; ARB, angiotensin-receptor blocker; BB, beta-blocker; CVD, cardiovascular disease; CKD, chronic kidney disease; MI, myocardial infarction. aNot considered “compelling” indication in JNC-7 Express guidelines. bNot considered “compelling” recommendation in ACCF/AHA recommendations. Source: Journal of the American College of Cardiology by American College of Cardiology. Reproduced with permission of Elsevier Inc. in the format Journal via Copyright Clearance Center. | ||||||
Recent guidelines from ASH describe combination therapies of hypertension in categories of preferred, acceptable, and less effective, based on efficacy in lowering BP, safety and tolerability, and certain known outcomes from longer-term trials (TABLE 3).47
TABLE 3
Drug combinations in hypertension: Recommendations from the American Society of Hypertension47
| Preferred | Acceptable | Less Effective |
|---|---|---|
| ACEI + diuretica | BB + diuretica | ACEI + ARB |
| ARB + diuretica | Calcium antagonist + diuretic | ACEI + BB |
| ACEI + CCBa | Renin inhibitor + diuretic | ARB + BB |
| ARB + CCBa | Renin inhibitor + ARBa,b | CCB (non-dihydropyridine) + BB |
| Thiazide diuretic + potassium-sparing diuretica | Centrally acting agent + BB | |
| ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker; BB, beta-blocker; CCB, calcium channel blocker. aAvailable as single-pill combination. bThis may be medically inappropriate in patients with diabetes and chronic diabetic nephropathy. Source: Journal of the American Society of Hypertension: JASH by American Society of Hypertension. Reproduced with permission of Elsevier Inc. in the format Journal via Copyright Clearance Center. | ||
In 2010, the American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) published an expert consensus document on hypertension in the elderly. It recommends single therapy or combination therapy with an ACEI, ARB, calcium antagonist, or diuretic for patients 65 years of age and older with stage 1 hypertension and no “compelling” indications (eg, HF, post-MI, known coronary disease, angina, aortopathy/aortic aneurysm, diabetes, recurrent stroke prevention, chronic kidney disease, and early vascular dementia), but combination therapy for those with stage 2 hypertension and no compelling indications. For the former group, the panel notes that the combination of amlodipine with a renin-angiotensin aldosterone system blocker may be preferable to a diuretic combination, although either is acceptable.41
For patients with compelling indications, the ACCF/AHA panel recommends condition-based combination therapy with 2 or more of the therapies summarized in TABLE 2.41,49 The panel’s algorithm for the management of hypertension in the elderly is depicted in FIGURE 2.41
FIGURE 2
ACCF/AHA algorithm for the management of hypertension in the elderly41
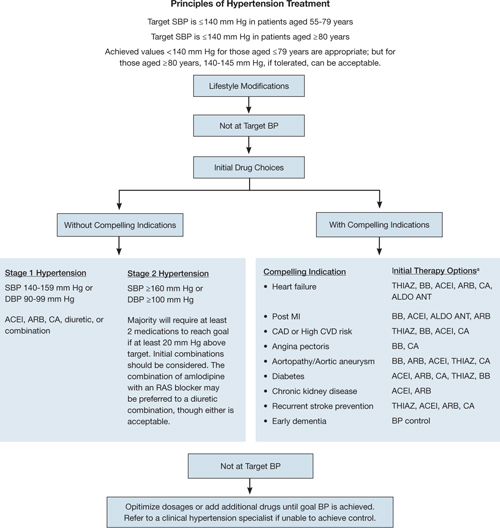
ACCF, American College of Cardiology Foundation; ACEI, angiotensin-converting enzyme inhibitor; AHA, American Heart Association; ALDO ANT, aldosterone antagonist; ARB, angiotensin II receptor blocker; BB, beta-blocker; BP, blood pressure; CA, calcium antagonist; CAD, coronary artery disease; CVD, cardiovascular disease; DBP, diastolic BP; MI, myocardial infarction; RAS, renin-angiotensin system; SBP, systolic BP; THIAZ, thiazide diuretic.
aCombination therapy.
Source: Journal of the American College of Cardiology by American College of Cardiology. Reproduced with permission of Elsevier Inc. in the format Journal via Copyright Clearance Center.The National Institute for Health and Clinical Excellence (NICE), the United Kingdom-based clinical guideline development organization, recommends in its 2011 guidelines for the clinical management of primary hypertension in adults that patients less than 55 years of age, not of black African or Caribbean heritage, begin treatment with an ACEI or ARB.50 The guidelines do not recommend beta-blockers for initial therapy, noting that they should be considered only in younger patients with intolerance or contraindications to ACEIs and ARBs, reproductive-aged women, and those with clinical evidence of increased sympathetic drive.50
In contrast, patients 55 years and older, or blacks of African or Caribbean origin of any age, should begin treatment with a calcium channel blocker (CCB).50 If they cannot tolerate a CCB, or for those with HF (or at high risk of HF), the guidelines recommend beginning therapy with a diuretic (preferably chlorthalidone or in-dapamide unless the patient’s hypertension is already controlled with bendroflumethiazide or HCTZ).
If initial treatment fails to lower BP adequately, step 2 of the NICE guidelines for all populations is treatment with an ACEI or ARB in combination with a calcium antagonist.50 If further therapy is necessary (step 3), a thiazide diuretic (or thiazide-like) should be added to that combination. It is also recommended that patients with drug-resistant hypertension (ie, taking 3 agents at maximally tolerated doses, 1 of which should be a diuretic) should receive additional treatment with low-dose spironolactone (if their serum potassium level is ≤4.5 mmol/L) and higher-dose thiazide-type diuretics (if their serum potassium level is >4.5 mmol/L). If the diuretic is not tolerated or is ineffective, an alpha- or beta-blocker may be added. If patients continue to exhibit continued resistance, NICE recommends referral to a hypertension specialist. The NICE algorithm for the treatment of hypertension is shown in FIGURE 3.50