As psychiatrists, we understand that behavior is complex and determined by multiple factors. However, despite our understanding that behavior is cultural, sociological, psychological, and biological, we often lose sight of the biological perspective because the brain is such a complex organ and because we are inundated with psychological theories of behavior. As I have said before, we cannot abdicate our role of being biologists in the reflection of mental health and wellness.
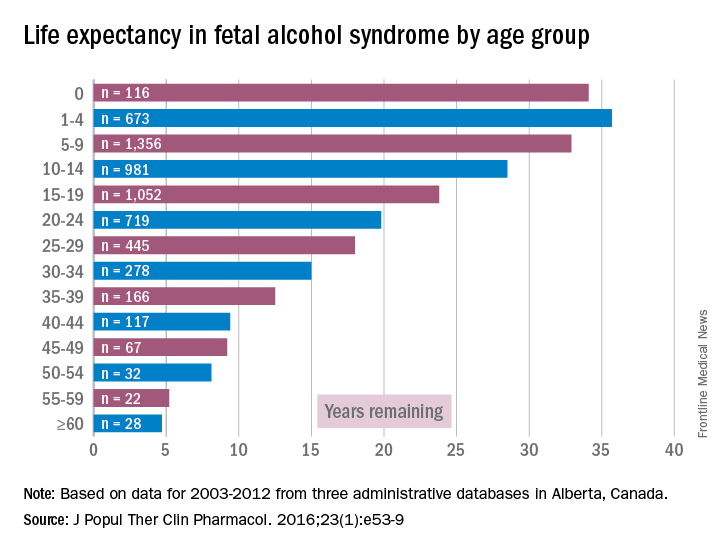
Accordingly, I feel it is my duty to bring our attention to a biologic etiology of suicidal behavior. I came across an article on the life expectancy of individuals afflicted with fetal alcohol syndrome in the Journal of Population Therapeutics and Clinical Pharmacology (2016;23[1]:e53-9). The findings were astonishing. As it turns out, the life expectancy of people with fetal alcohol syndrome is 34 years of age on average, and the leading causes of death were “external causes,” which accounted for 44% of the deaths. Suicide was responsible for 15% of those deaths, accidents for 14%, poisoning by illegal drugs or alcohol for 7%, and other external causes for another 7%, according to the article.
Anyone who has been following my commentaries in Clinical Psychiatry News will know that I have become interested in an invisible public health problem of fetal alcohol spectrum disorders, which are being proposed as a new diagnosis of neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE) in the DSM-5. My interest has been spurred by the problem of affect dysregulation that these patients exhibit. My analysis of this dynamic is that affect dysregulation causes these patients to engage in a plethora of risky behaviors that cause morbidity and mortality, including drug use, violence, and unsafe sex. Now, the research by N.X. Thanh and E. Jonsson mentioned above is leading me to add suicide attempts to that list.While working in a general hospital in a low-income African American environment where there are high rates of fetal alcohol exposure, I see at least 3-4 suicide attempts a week on the medical-surgical/psychiatric inpatient units where I serve. I am always looking for patients who have ND-PAE because determining such a diagnosis is critical to those patients’ medical-surgical care. For example, there was one woman with ND-PAE who had operable breast carcinoma but did not come in for a return visit until after her carcinoma had become inoperable (she forgot how important it was to get timely treatment). There was a patient who always had out-of-control diabetes because he did not know how to use his glucometer. There was a patient who was taking his antipsychotic medication during the day instead of as prescribed – at bedtime – because he could not read the instructions on his medication bottle. (I have altered several key aspects of my patients’ stories to protect their confidentiality.)
However, until I read that suicide was responsible for 15% of deaths with external causes among patients with fetal alcohol syndrome – patients whose life expectancy averages only 34 years – it did not occur to me that affect dysregulation also was likely to lead to suicide attempts among patients with ND-PAE.
One patient in particular brought the point home. She was frequently in the hospital for suicide attempts after arguments with her boyfriend. The first time I saw the patient, her fetal alcohol spectrum disorder diagnosis was apparent: She was born premature, with a low birth weight, and with vestiges of fetal alcohol facies. Her problems began in childhood; she was in special education in school. As an adult, she could barely hold a job for longer than a week, and she had problems with affect regulation. Of course, she was diagnosed as having bipolar disorder for “mood swings” that could last less than a day. Her grandmother had told the patient that her mother was drinking and using drugs while pregnant with her. After attempting suicide for the third or fourth time in a year, the patient was admitted for suicidal behavior to Jackson Park Hospital, and the biological etiology of her suicidal behavior became clear to me.When several of us who were working on the issue of suicide prevention while part of the Committee on Psychopathology & Prevention of Adolescent & Adult Suicide produced our report called “Reducing Suicide: A National Perspective” in 2002, the idea that paying attention to fetal environments and birth outcomes could inform the area of suicide prevention was an alien one. Now, it is a serious consideration because this dynamic just might explain part of the complex phenomena of some suicidal behaviors.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital Family Medicine Clinic in Chicago; clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago; former president/CEO of Community Mental Health Council; and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago.