PHILADELPHIA – A blood glucose target of 121-180 mg/dL for patients following isolated coronary bypass surgery was as clinically effective as was a stricter glucose target and was easier to maintain in a randomized study with 189 patients.
Based on these results, the cardiac surgery program that ran the study switched its blood glucose range for postoperative patients from 90-120 mg/dL to the more liberal range of 121-180 mg/dL, Dr. Shalin P. Desai said at the annual meeting of the American Association for Thoracic Surgery.
"We believe that maintaining patients at a blood glucose level less than 180 mg/dL is safe and effective, and therefore should be considered for patients undergoing coronary artery bypass grafting surgery," said Dr. Desai, a cardiac surgeon at Inova Heart and Vascular Institute in Falls Church, Va.
"We know that a glucose level of less than 180 mg/dL is good, but does it need to be so strict that it’s almost normoglycemic, or can it be more liberal when we know the glucose levels will rise with the stress of surgery and illness? A range of 121-180 mg/dL is probably sufficient," Dr. Desai said in an interview. At that level, "we used less insulin, fewer finger sticks, and fewer resources" than when the target range aims for lower blood glucose levels, he said.
Dr. Desai and his associates enrolled patients undergoing first-time, isolated CABG who had diabetes or required insulin treatment following surgery based on having three consecutive blood glucose readings of at least 150 mg/dL, or one reading of at least 200 mg/dL. The researchers used a bedside, computerized device that regularly assessed blood glucose levels and adjusted the insulin infusion accordingly. The patients averaged 62 years of age, and about 43% had diabetes.
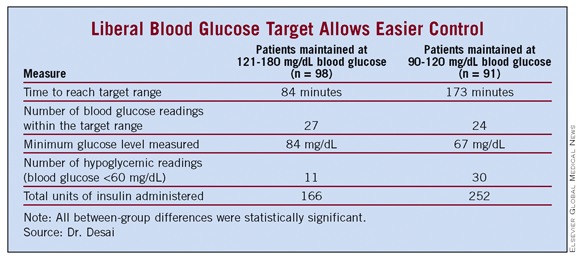
Among the 98 patients maintained on the 121-180 mg/dL regimen, the average time needed to reach the target blood glucose range was 84 minutes – significantly shorter than the average 173 minutes needed for the 91 patients on the strict regimen.
Patients maintained on the liberal target also fared significantly better in their average number of readings within their target range, minimum glucose level, number of hypoglycemic readings, and total insulin dose received (see table).
Assessment of clinical outcomes – renal failure, atrial fibrillation, pneumonia, deep sternal wound infections, prolonged ventilation, prolonged hospitalization, and operative mortality – showed that the liberal range was not inferior to the strict range for preventing these complications in the primary, intention-to-treat analysis. In the as-treated and per-protocol analyses, the liberal-range patients had outcomes that were noninferior to those of the strict control patients for all parameters except for atrial fibrillation. The liberal-range patients showed a small excess of atrial fibrillations in these two additional analyses.
Future studies should look at the same issue in patients undergoing other types of cardiac surgery, such as valve repair or replacement, or a maze procedure, he said.
Dr. Desai said that he had no relevant financial disclosures.