H. L. Mencken was a 20th century journalist and critic who provided us with a number of great quotes. One of my favorites is:
“There is always an easy solution to every human problem—neat, plausible, and wrong."1
I like this quote because it applies to many aspects of pain. In this and upcoming issues of Chronic Pain Perspectives, we examine why chronic pain needs to be viewed as a complex situation that affects the mind, body, and soul of our patients, one in which the simple, neat solution is often not enough. Although we may wish to “tackle” pain as we would an objective value and reduce it with a unimodal approach, experience and several lines of research demonstrate that we are positioning ourselves, and our patients, for disappointment. The problem here is not in our patients, but in the fact that their pain is not a discrete entity. Pain is a doorway into a sequela of suffering that needs to be appreciated and addressed if we have any hope of helping our patients return to functionality.
Pain does not travel alone
The research guides us to understand that when there is pain, there are current or emerging issues with mood, energy, cognition, and function. Although depression is found in approximately 10% to 15% of all patients seen in primary care, those who have chronic pain have been found to present with depression as much as 58% of the time,2 making it the most common psychiatric comorbidity. Conversely, in a large study of primary care patients with major depressive disorder, chronic pain was present nearly 66% of the time.3
Beyond depression, the patient with chronic pain is more likely to have coexisting anxiety,3 panic,3 sleep dysfunction characterized by sleep maintenance insomnia and fatigue,4 restless leg syndrome,4 and loss of gray matter density that may be reversible.5,6 This brings up the age-old intellectual question, “Which came first?” What we appreciate more and more—through understanding the common pathophysiological mechanisms seen in conditions such as migraine, depression, and cardiovascular disease,7—is that these disorders are co-developing and making their way into the chief complaint in various layers and word choices.
Pain does not stay in the same silo
As we focus more closely on pain as a foe that we can subdue, we find that it exerts an influence on many “friends,” and that pain and its elusive friends have the ability to jump from one arena into another, sometimes making the battle feel insurmountable. Recent research points this out; in a 30-year study of headache, over the course of their illness patients were found to switch from their initial diagnosis of headache type to other headache diagnoses more than 80% of the time.8[Figure]
FIGURE: Combinations of headache subtypes across 30 years among participants
who met criteria for migraine or tension-type headache (n=346)
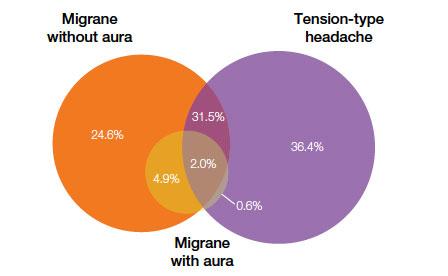
Source: Adapted from Merikangas KR, et al. Magnitude, impact, and stability of
primary headache subtypes: 30 year prospective Swiss cohort study. BMJ. 2011;343:d5706
What this creates is the awareness that we are not really fighting a single condition, but a complex picture of suffering, and that we must take into account many layers of the patient who presents to us. In this way we can push past the simple but disappointing solution to a more integrative, individualized, complex one that holds the potential for relief on multiple levels.
I’ll leave you with another Mencken quote that offers sage advice in this regard:
“The essence of science is that it is always willing to abandon a given idea, however fundamental it may seem to be, for a better one.“9