TABLE
Heart failure: Ejection fraction status dictates treatment6-8
| Intervention | Indications in patients with reduced EF (evidence supporting its use) | Indications in patients with preserved EF (evidence supporting its use) |
|---|---|---|
| ACEIs | •All patients (reduced mortality) | No evidence |
| Beta-blockers | • All symptomatic patients (reduced mortality) | No evidence |
| Aldosterone antagonists | • Rest dyspnea • Post-MI with diabetes or symptomatic HF (reduced mortality) | No evidence |
| Nitrates | • African American patients with persistent symptoms despite treatment with ACEIs, beta-blockers, and diuretics • Intolerance to ACEI/ARBs due to renal impairment (reduced mortality) | No evidence |
| Diuretics | As needed for fluid overload | As needed for fluid overload |
| ARBs | • Intolerance to ACEIs due to cough • Consider for patients with ACEI intolerance due to angioedema* (reduced mortality) | Symptomatic patients (reduced hospitalization rates) |
| Digoxin | • Persistent symptoms despite background therapy • HF and atrial fibrillation (reduced hospitalization rates) | No evidence |
| ICDs | • EF <35% and ischemic cardiomyopathy or symptomatic HF (reduced mortality) | No evidence |
| *There is a possibility of cross-reactivity. | ||
| ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; EF, ejection fraction; HF, heart failure; ICDs, implantable cardioverter defibrillators; MI, myocardial infarction. | ||
How to treat the patient with normalized EF
These 2 options, however, do not clearly address the question of what to do with patients like Joe, whose case is described in our opener. Should patients whose EF has normalized after months, or years, of aggressive treatment remain on the medication regimen they followed when they had reduced EF? Should they be treated as HF patients with preserved EF? Is there another option? How often should patients who initially had a reduced EF be reassessed? To answer these questions, let’s take a closer look at the evidence.
Measurement of EF. No large clinical trials have investigated the impact of serial measurement of EF. Two small studies showed prognostic significance with serial measurements that demonstrated improvements in EF,11,12 but their reproducibility and clinical significance are unclear. The American College of Cardiology/American Heart Association and the European Society of Cardiology recommend repeat measurement of EF only when it is clinically indicated.6,13
Accuracy of the results. Echocardiogram is among the most widely used cardiac imaging modalities because it is fast, portable, and noninvasive. However, physiologic limitations and the challenges of calculating a 3-dimensional parameter with 2-dimensional images (FIGURE) limit the usefulness of echocardiography for the measurement of EF. Among other things, echocardiography lacks the ability to reliably identify small changes or improvements. Newer techniques—such as contrast or radionuclide ventriculography—have shown improved reliability in early studies.14 Compared with echocardiography, however, ventriculography is more costly and more invasive.
McGowan et al15 conducted a systematic review of studies comparing echocardiography with reference standards of contrast or radionuclide ventriculography. They concluded that no method in general use to calculate EF from echocardiographic images could provide a 95% confidence interval (CI) of <±10% in the measurement of EF. The American Society of Echocardiography has published standards to improve measurement technique and minimize variability in EF measurement.16
FIGURE
Echocardiographic evidence of heart failure? Systolic image tells the story
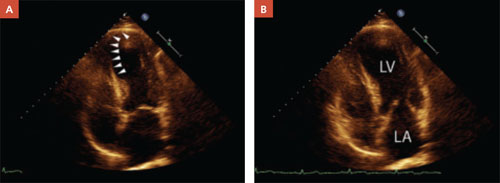
In a patient with reduced ejection fraction, the systolic image (A) reveals septal apical akinesis (arrows) and hypokinesis in the remainder of the left ventricle. The diastolic image (B) is unremarkable.
Normalization of EF is not a cure
In treating patients with HF, it is crucial to distinguish between what is reversible and what is not. Diuretics, oxygen, and other supportive therapy may reverse symptoms of congestion. Reversible causes of HF may include alcohol toxicity, thyroid disease, tachycardia, anemia, valvular heart disease, and CAD, among others. However, reversing the symptoms or the cause does not necessarily reverse HF itself. Further, normalization of EF does not necessarily imply that HF has been cured.
In a prospective study of 42 HF patients whose EF had normalized, the aggregate initial EF was 26%. It increased to ≥40%, with an absolute increase in EF ≥10%. During 41 months of follow-up, 19% of the patients had a recurrence of reduced EF. The likelihood of recurrence was greater among those who had discontinued their HF medications, the researchers found.17
In another prospective study, researchers followed 110 patients with reduced EF who were managed medically according to guideline-prescribed therapy.18 During a 17-month follow-up period, 18% had a normal EF at some point—but in more than half the cases (55%), the improvement was transient. Factors that were predictive of normalization included the presence of arterial hypertension (odds ratio [OR]=8.5; P=.01), nonischemic etiology (OR=4.9; P=.02), the absence of diabetes (OR=9.5; P=.01), beta-blocker therapy with carvedilol (OR=3.9, P=.02), and a higher beta-blocker dosage (OR=1.1; P=.04). Normalization occurred, on average, at 13 months (±6 months). The only difference between those who had a sustained improvement and those for whom the normalization was transient was the rate of chronic obstructive pulmonary disease (COPD). None of the patients who had a sustained improvement had COPD; 36% of those with transient improvement did (P=.04).