Arthrography
Arthrography was the diagnostic test of choice before MRI. It is specific for rotator cuff tears but lacks sensitivity15 because it cannot detect partial-thickness or associated soft tissue injuries of the shoulder. Arthrography still has a role in evaluating adhesive capsulitis by demonstrating decreased intracapsular volume.26 The test can be therapeutic if the capsule is dilated during the procedure. Additionally, patients with claustrophobia may be good candidates for arthrography if a full-thickness tear is suspected and MRI is not possible.
Computed tomography
Computed tomography may be used to evaluate bony lesions, including glenoid rim fractures, humoral fractures, and acromioclavicular joint disease. Computed tomography arthrograms may have a role in assessing labral tears and full-thickness rotator cuff tears.35 The use of CT arthrography has fallen into disfavor compared with MRI because of the risks associated with contrast exposure and poor sensitivity for partial-thickness rotator cuff tears or associated soft tissue injury.
Ultrasound
Ultrasound has been used in the evaluation of rotator cuff tears with varying degrees of sensitivity and specificity.12,29,34 This inconsistency may be related to variation in operator skill. Advantages of US include relatively low cost, speed, and noninvasiveness.
Magnetic resonance imaging
Magnetic resonance imaging has become the gold standard for diagnostic imaging of the shoulder related to soft tissue injury. The advantages include its noninvasive nature, lack of contrast exposure, nonionizing radiation, high degree of resolution, and the ability to evaluate multiple potential pathologic processes.36 Magnetic resonance imaging is the preferred test for evaluating impingement syndrome and rotator cuff pathology. A normal MRI greatly reduces the chances of a rotator cuff tear, with a negative likelihood ratio of 0.08.16,29,30 Magnetic resonance imaging is also useful in the evaluation of avascular necrosis, biceps tendon disorders, inflammatory processes, and tumors.13 The diagnosis of labral lesions can be challenging given the relatively low sensitivity and negative predictive value noted in several trials.16,28,31 Finally, it is important to note that up to one third of all asymptomatic patients and more than half of those older than 60 years demonstrate asymptomatic rotator cuff tears on MRI.37
Approach to the patient
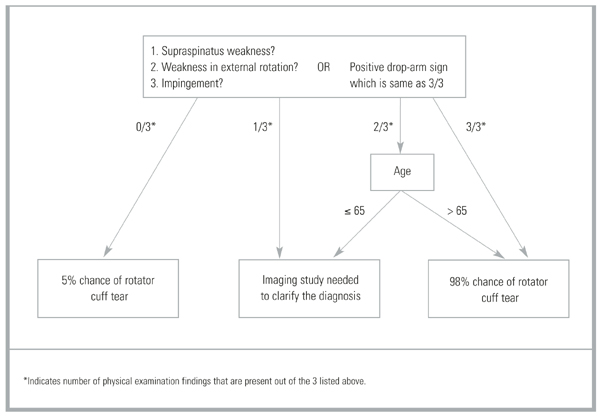
A general approach to the patient with shoulder pain is summarized in Figure 5. Pre- and posttest probabilities are included to give an understanding of how tests may help diagnose or rule out a complete rotator cuff tear. A recent prospective study combining multiple examination maneuvers demonstrated that a combination of 3 physical examination findings (supraspinatus weakness, weakness in external rotation, and impingement) along with the patient’s age can often diagnose or rule out a rotator cuff tear.38 This group of tests did not distinguish full versus partial thickness tears. This approach is summarized in Figure 6.
Figure 5
Basic approach to assess for complete rotator cuff tear

Figure 6
Alternative approach to a suspected rotator cuff tear