The Applied Evidence article on the evaluation of shoulder pain by Stevenson and Trojian1 in the July 2002 issue of The journal of family practice was practical and useful. It can not be stressed enough how knowing the implications and limits of physical examination maneuvers can help lead us to or away from a particular diagnosis.
It was surprising that the authors did not discuss the usefulness of magnetic resonance (MR) arthrography in the diagnostic tests section of the article. MR arthrography can be superior to MR imaging when evaluating certain capsular/labral pathologies and incomplete rotator cuff tears.2,3 Chandnani and colleagues4 studied the same shoulders with conventional MR imaging and MR arthrography. The accuracy of each imaging technique for different parts of the labral/ligamentous complex is shown in the Table.
Franklin Sease, MD, and Stephen A. Wilson, MD,
UPMC St. Margaret, Pittsburgh, Pa.
E-mail: seasewf@msx.upmc.edu, wilsons2@msx.upmc.edu
TABLE
| Condition | Sensitivity | Specificity | LR+ | LR- |
|---|---|---|---|---|
| Labral tear | ||||
| Conventional MR | 93 | 100 | > 20 | 0.07 |
| MR arthrogram | 96 | 100 | > 20 | 0.04 |
| Detached fragment | ||||
| Conventional MR | 46 | 100 | > 20 | 0.54 |
| MR arthrogram | 96 | 75 | 3.9 | 0.05 |
| Labral detachment | ||||
| Conventional MR | 11 | 83 | 0.7 | 1.1 |
| MR arthrogram | 56 | 83 | 3.3 | 0.53 |
| LR+, positive likelihood ratio; LR-, negative likelihood ratio; MR, magnetic resonance | ||||
Drs. Stevenson and Trojian respond:
Drs. Sease and Wilson make excellent points in their letter regarding our article. The omission of MR arthrograms was due to limits on the length of the article rather than a lack of importance of the test. We agree that at least 2 small studies have demonstrated some increased sensitivity of MR arthrograms compared with plain MR imaging for labral tears.4,5 The effect of MRI arthrography on clinical outcomes is not clear, though, and an MRI arthrogram is invasive, causes discomfort with needle placement, and exposes the patient to the potential for an adverse reaction from the contrast.6
Given the risks and the limited benefit in regards to increased sensitivity,4-8 we reserve MR arthrograms for a small subset of our patients who have persistent signs or symptoms of a labral tear despite a negative MRI. We also use them with athletes where the need for an immediate and accurate diagnosis outweighs the risks. We do not routinely use an MR arthrogram for rotator cuff tears since a thorough history and physical, followed by a plain MRI, is often sufficient to make a diagnosis of either a partial or complete tear.1
J. Herbert Stevenson, MD,
Department of Family Practice,
University of Massachusetts, Fitchburg.
E-mail: stevenson70@yahoo.com.
Thomas H. Trojian, MD,
Department of Family Medicine, University of Connecticut/Saint Francis Hospital and Medical Center,
Hartford.
E-mail: TTrojian@stfranciscare.org
Figure 1
Antimanic efficacy of olanzapine, 15 mg/d, in acute bipolar mania and mixed episodes
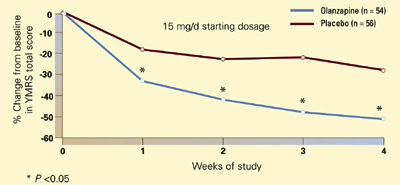
Patients with acute bipolar mania or a mixed episode were treated with olanzapine or placebo for 4 weeks in a randomized, double-blind trial. Compared with placebo, olanzapine at a starting dosage of 15 mg/d was associated with significant symptom improvement in the first week (50% change from baseline in Young Mania Rating Scale total score). This trend continued throughout the trial.
Source: Reprinted with permission from Tohen M et al. Arch Gen Psychiatry 2002; 57(9):841-9. Copyright 2002. American Medical Association