A 43-year-old Caucasian male presented to the emergency department complaining of left lower quadrant pain that had lasted 1 day. He described the pain as “a wrench twisting my insides,” and he rated it as 8 out of 10. He also complained of nausea and non-bloody, nonbilious emesis. He did not have fever, chills, or weight loss. His medical history included diverticulitis, sigmoid colectomy, and nephrolithiasis.
The physical exam revealed a heart rate of 102 beats per minute, blood pressure of 153/89 mm Hg, respiratory rate of 20, and a temperature of 99.2°F. Abdominal exam demonstrated mild left lower quadrant tenderness to palpation without rebound or guarding. The remainder of the physical exam was unremarkable. Laboratory studies demonstrated a normal blood count and differential, and a normal comprehensive metabolic profile. The urinalysis showed 60–80 red blood cells per high-power field (RBC/HPF). A computed tomography (CT) scan of his abdomen revealed a 3-mm calculus in the mid-left ureter without hydronephrosis, and a few small descending colon diverticuli. The patient was treated conservatively with hydration, analgesics, and antiemetic medications.
Radiographic findings
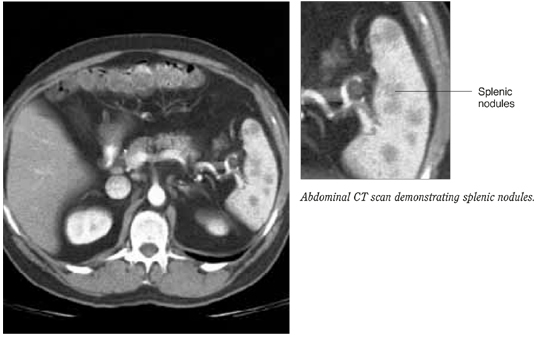
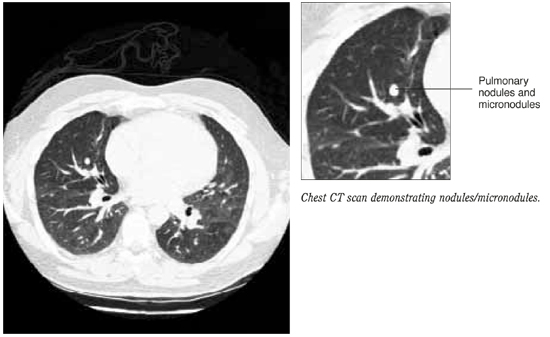
The following day, the radiologist called the patient’s primary care physician to report that upon rereading the abdominal CT scan there appeared to be “patchy enhancement of the spleen” (Figure 1). Follow-up abdominal ultrasound revealed multiple irregular areas of low density within the spleen. A CT-guided spleen biopsy discovered multiple noncaseating, non-necrotizing granulomas. Subsequent chest CT revealed multiple bilateral micronodules and nodules (Figure 2).
FIGURE 1
Abdominal CT scan
Chest CT scan
What are the management options?
What is the prognosis?