Is there a place for astringents?
Before antibiotic availability, the mainstay of treatment was topical compounds containing astringents such as aluminum acetate solution (Burow’s Solution USP, Domeboro, and others) and acetic acid solutions (Vosol Otic).14-16 These preparations are still widely used but principally to prevent otitis externa.
Topical 8% aluminum acetate solution was as effective as a commonly used antimicrobial-corticosteroid topical mixture (polymyxin-neomycin-hydrocortisone) for 25 adult patients with otitis externa (72% vs 76%, respectively).17 In a doubleblind, randomized study involving 65 adults and children, the effectiveness of aluminum acetate equaled that of gentamicin otic solution.18
In a Dutch study evaluating otitis externa in 213 adults, topical antibiotics were more effective than topical acetic acid alone and alleviated symptoms faster than acetic acid plus steroids.
The lack of a large, well-structured, placebo-controlled study or other compelling evidence casts doubt on the relative effectiveness of astringent topical treatments for otitis externa. Also, topical astringents are often painful, which may impede adherence.19
Practitioners usually reserve nonspecific therapy such as acetic acid and Burow’s solution for prevention and self-medication for mild symptoms. Studies that include measures of clinical goals, such as pain relief, cessation of symptoms, and eradication of infection, are needed before astringent agents can be recommended for routine therapy of moderate to severe otitis externa. Most treatment data concerning otitis externa have centered on therapy with antimicrobial otic drops.20
Preparing the ear for antibiotic administration
Topical antibiotics are presumed to eradicate pathogens most effectively through direct contact at concentrations exceeding the minimum inhibitory concentration (MIC90).21-23
Debride if possible. Though the severity of pain may preclude debridement, removing debris from the external ear canal during the office visit will maximize delivery of the medication. This can be performed with a dry cotton swab or small Calgiswab or by suctioning with a metal or plastic catheter. Cleansing by irrigation or flushing of the ear canal with a syringe or pulsatile irrigator (Water-Pik) may be more tolerable for some patients, but probably should be performed only when the tympanic membrane can be visualized due to the risk that the debris overlies an unseen perforation of the tympanic membrane.24
Ear wick helpful. After the ear canal has been debrided, consider the benefit of inserting an ear wick. Particularly if the ear canal is swollen, medication may not penetrate deep enough into the canal. In this situation, an ear wick, such as a Pope Oto-wick or Merocel XL (Medtronic Xomed, Inc, Jacksonville, Fla) hydrogel polymer, can enhance medication delivery directly to the entire ear canal.
The medication is absorbed into the ear wick, which delivers the drug to the infected skin (FIGURE). As swelling subsides, most ear wicks extrude spontaneously, usually within 12 to 36 hours. Once the edema subsides and much of the debris in the external ear canal has been cleared, topical antibiotics can be instilled.
FIGURE 1
Ear wick within the external ear canal
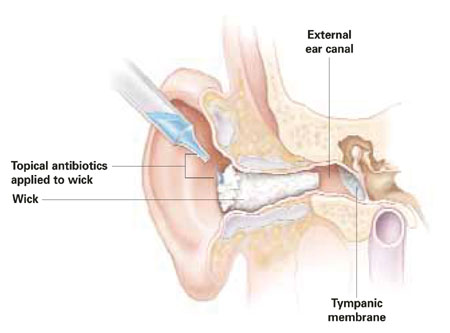
The ear wick is inserted into the external auditory canal until the remaining edge is flush with the external ear. In smaller children, one fourth to one third of the wick may be cut to prevent it from falling out prematurely. Several drops of topical antibiotics are instilled onto the wick until it has fully expanded. At home, a few drops of topical antibiotic should be applied to the wick every few hours for the first 24 hours to keep the wick moist. The wick should be removed with tweezers within 24 to 48 hours if it has not already fallen out.
Common topical therapies
Topical antibiotics commonly used for otitis externa are listed in the TABLE.
TABLE
Common topical antibiotic treatments for otitis externa
| TREATMENT (FORMULATION) | DOSING REGIMEN | ADVANTAGES/DISADVANTAGES |
|---|---|---|
| Neomycin sulfate/polymyxin B/hydrocortisone (suspension/acidic) | 4 times daily | Efficacious, extensively used; moderately expensive (AWP $65) |
| Resistance and hypersensitivity increasing; potentially ototoxic; discourages compliance | ||
| Ofloxacin otic (solution/neutral) | Once or twice daily | Efficacious; no ototoxicity or hypersensitivity; favors compliance |
| Resistance increasing; moderately expensive (AWP 5 cc $44.45; 10 cc $82.25) | ||
| Ciprofloxacin otic, with dexamethasone (suspension/acidic) | Twice daily | Efficacious; no ototoxicity with ciprofloxacin; favors compliance |
| Resistance increasing; expensive (AWP $85) | ||
| AWP, average wholesale price | ||
Combination drugs containing aminoglycosides
Combination topical drugs containing an aminoglycoside (neomycin), polymyxin B, and a corticosteroid were once the only antibiotic treatments for otitis externa approved by the US Food and Drug Administration.9 Neomycin is a bactericidal inhibitor of protein synthesis that is modestly active against S aureus but has minimal activity against P aeruginosa.25
In 1999, a prevalence study of aminoglycoside resistance in Europe found that 25% of the S aureus isolates tested were resistant to gentamicin.26 This study also found a high incidence (20%–38%) of gentamicin-resistant P aeruginosa isolates from Belgium, France, Italy, and Poland.26 Furthermore, in a prospective study of aural isolates of P aeruginosa, only 17.8% were susceptible to neomycin.27