Data synthesis
The studies we reviewed were judged clinically to be too heterogeneous to support a quantitative synthesis; therefore, our review is narrative. However, to promote the comparison of results across studies we extracted outcome data in a common format and present it in graphs for visual comparison. For studies that reported on both 1-hour and 2-hour postprandial blood glucose levels, we chose the 2-hour measurement for the analysis. For studies that reported more than 1 follow-up time, we selected the follow-up time that was closest to 3 months.
Twenty-two studies were selected for further analysis based on the criteria described above. These studies represented either RCTs (2) or CCTs/natural experiments (5) with a comparison arm that did not receive an herb, or studies that had pre/post comparison data available (8).
We considered 2 subgroups of eligible studies separately: the RCTs and CCTs or natural experiments that had nonherbal/Ayurvedic comparison arm(s) were considered 1 subgroup, and all other eligible (pre/post data available) studies made up the second subgroup. The RCT/CCT/natural experiments subgroup allowed us to do a comparison between herbal and nonherbal arms within a study, providing a stronger level of evidence than pre/post comparisons. For these studies, we were able to compare the effects of different treatments after the placebo or nonherbal arm results were taken into account by estimating a difference of differences statistic and its 95% confidence interval. This statistic is equal to the difference between the pre- and post-treatment means in the Ayurvedic arm minus the analogous difference in the nonherbal/Ayurvedic arm. The pre/post studies subgroup did not allow a concurrent comparison, but the difference between pre- and post-treatment means could be estimated along with a 95% confidence interval.4 Further details are given in our Evidence Report (available online at www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat1.chapter.95372).
For each study subgroup, we assessed the possibility of publication bias graphically by evaluating a funnel plot of the study summary statistics for asymmetry, which would result from the nonpublication of small trials with negative outcomes. Because graphical evaluation can be subjective, we also conducted an adjusted rank-correlation test9 and a regression asymmetry test10 as formal statistical tests for publication bias.
Results
Description of the evidence
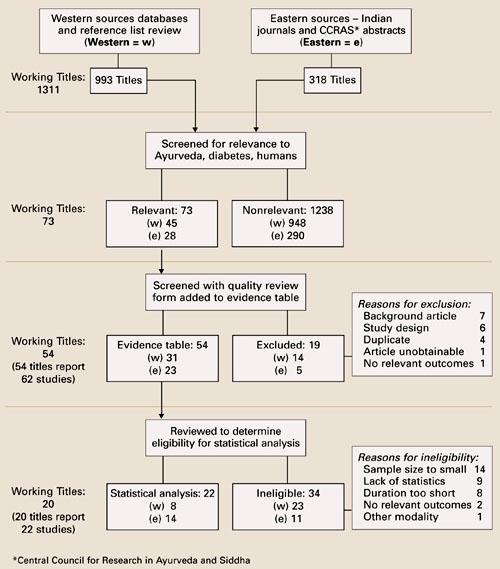
As a result of our search, we considered a total of 1311 articles (FIGURE 1). We reviewed in depth 62 studies, of which 22 were analyzed statistically. Ten studies came from the Western literature, and 12 came from the Indian literature. There were 7 randomized controlled trials, controlled clinical trials, or natural experiments with a treatment/no treatment comparison. There were 15 case series or cohort studies using a “pre/post” analysis. TABLE W2 (available online at www.jfponline.com) summarizes the characteristics of studies.
In terms of interventions, there was no study that tested Ayurveda as a system of care; all tested herbs. Of the 22 studies described narratively in this article, the 2 most commonly tested single herbs were Coccinia indica and fenugreek. The Ayurvedic formula Ayush-82 was the most commonly tested herbal formula. Diet was used as an intervention or co-intervention in 15 of the 22 studies.
FIGURE 1
Ayurveda literature review strategy of focused search for human diabetes articles
Quality of the evidence
Only the RCTs, CCTs, and natural experiments were given a Jadad score, which rates studies on a 0 to 5 scale.5 Of the 7 such studies, 3 received a Jadad score of zero, 3 studies scored a 1, and only 1 study received a 4 on this scale. This is the only high quality study in our analysis.
Controlled trials/natural experiments with nonherbal comparison arm(s)
There were 7 RCTs, CCTs or natural experiments that met the inclusion criteria. The data for these 7 studies are reported in FIGURE 2.
Coccinia indica. Azad Khan, Akhtar, and Mahtab (1979) performed a randomized controlled trial to assess the hypoglycemic properties of a preparation of the herb C indica on uncontrolled and untreated type 2 diabetes patients.11 Thirty-eight patients with type 2 diabetes who were attending the outpatient department of the Bangladesh Institute of Research and Rehabilitation in Diabetes in Dhaka, Bangladesh, were recruited for the study. Only uncontrolled or newly diagnosed patients were enlisted. The intervention consisted of a freeze-dried powder of crushed leaves of C indica, given in a dose of 900 mg twice a day for 6 weeks. Control patients received placebo twice a day for the same period. Of the 16 patients receiving C indica, 10 patients showed a marked improvement in the glucose tolerance tests to values closer to normal, while none in the placebo arm showed marked improvement. The Jadad score for the trial was 4. This study was identified from the Eastern literature search.