A patient’s answer predicts outcomes. Another question is whether suicide ideation needs to be assessed over and above diagnosing psychiatric disorders such as major depression or alcohol abuse. A detailed analysis of the severity of suicide ideation is needed since it is the strongest predictor of successful suicide by patients with major depression.3 Furthermore, severe suicide ideation may affect time to treatment response4 and thus can influence decisions about duration of treatment.
Impact on mortality unknown. A important question regarding the impact of assessing suicide ideation is whether it reduces mortality. The US Preventive Services Task Force12 identified no study directly examining this concern.
Will your assessment of risk improve a patient’s outcome?
Evidence regarding the efficacy of antidepressant medications and psychotherapy in reducing risk for suicide is limited due to the methodologic and ethical difficulties associated with studying suicide. In a systematic review of intervention studies, Gaynes et al12 reported inconsistent findings of whether treating at-risk individuals reduces the number of suicide attempts or completions.
Interventions do, however, reduce suicide ideation, depression severity, and hopelessness, and do improve functioning.12,25,26 In the only study specifically targeting elderly depressed primary care patients, management of depression combined with antidepressant medication or psychotherapy reduced suicide ideation significantly more frequently than usual care.27
SSRIs and suicide. A continuing controversy is the relationship between selective serotonin reuptake inhibitors (SSRIs) and suicide attempts; a relationship possibly due to these drugs’ potential for agitation and akathasia. A review of randomized controlled trials documented a more than twofold increase in nonfatal suicide attempts among patients receiving SSRIs in comparison with placebo.28 A similar risk level was detected when comparing SSRIs and tricyclic antidepressants.28
Suicide attempts seem to increase during the first 1 to 9 days after treatment is started.29 This suggests that SSRIs do not immediately resolve depression or suicide ideation and may possibly increase risk in the first weeks of treatment. Closely monitor patients who are started on SSRIs, for symptom severity and suicide ideation (SOR: C).
Patient contracts. Suicide prevention contracts are often used to ensure that patients inform a family member or a healthcare professional if they no longer feel able to resist their suicidal thoughts. However, studies of suicide victims and attempters have found that many such patients had such a contract in place before the suicidal act.30,31 Thus, the American Psychiatric Association’s Practice Guideline for the Assessment and Treatment of Patients with Suicidal Behaviors3 cautions that suicide prevention contracts should not substitute for ongoing assessment of suicide ideation.
Targeting your assessment and management
Given the above knowledge base, physicians have been urged to help prevent suicide through targeted assessment and management.32,33 The Canadian Task Force on Preventive Health34 and the US Preventive Services Task Force12 recommend assessing suicide risk for primary care patients experiencing major depression or substance abuse (SOR: B).
Assessment may also be appropriate for those with panic disorder or a past suicidal attempt, and for those facing life-threatening illnesses, other stressful situations, or transitional life changes (SOR: C).
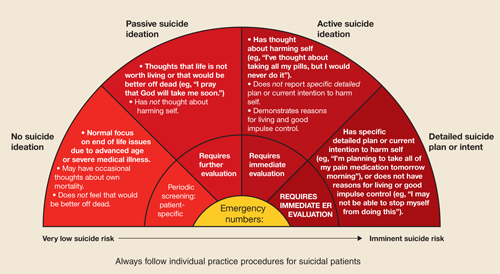
In this next section, we offer a structured assessment that identifies successive levels of suicide risk and advise corresponding action steps (FIGURE 1).35 The related visual tool (FIGURE 2), developed to improve depression detection by home care nurses,36 is pertinent for primary care clinicians as well.
FIGURE 1
Sequential questions to determine level of suicide risk
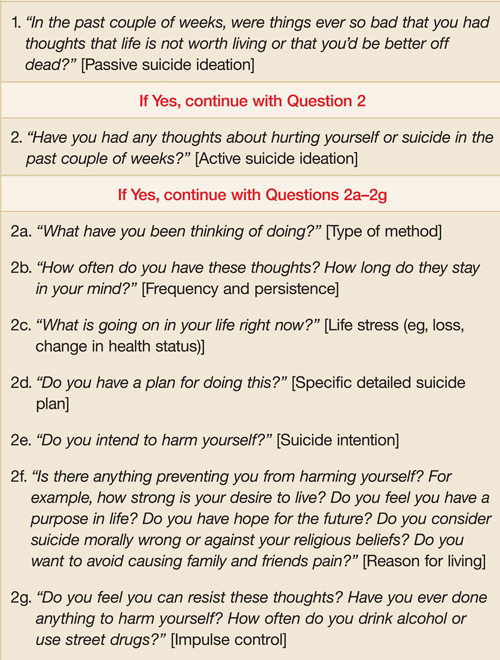
FIGURE 2
Suicide risk as a spectrum: Assessment and intervention strategies
Assessing suicide risk as a spectrum
Patient stigma, negative family and societal attitudes, and clinician discomfort can make depression and other emotional symptoms hard to talk about and impede appropriate screening.37 This makes identifying suicide ideation all the more difficult. When should you screen, and how should you ask clinical questions?
Screening instruments can help. Posing questions about suicide can be especially difficult during an initial visit. Therefore, you may administer a structured screening instrument such as the Patient Health Questionnaire (PHQ-9),38 the Beck Depression Inventory–Primary Care version (BDI-PC),39 or the Scale for Suicide Ideation (SSI).40 Alternatively, you may use the brief clinical interview format proposed here (see also Hamilton41 and Frierson et al42).
Spontaneous lines of questioning. When a patient’s particular circumstance leads to a discussion of pain, the impact of disability, social history, or difficulties coping, it would seem only natural for you to proceed to an assessment of emotional symptoms. You may begin with questions about mood and other depressive symptoms, and then specifically inquire about suicide ideation.
Older adults and patients whose ethnic and cultural backgrounds are different than yours may be particularly challenging. Recognize a particular group’s attitudes about suicide and revealing suicide ideation, and adapt assessment strategies accordingly. With older patients, for example, end-of-life discussions may serve as a way to elicit thoughts about death and dying.43