Practice recommendations
- The true origin of the heel pain of calcaneal apophysitis is a stress microfracture (invisible on x-ray) due to chronic repetitive microtrauma—it’s an overuse syndrome that resolves without surgery in nearly all cases. (C)
- Most patients experience pain relief and can resume full activities while using a simple in-shoe wedge-shaped orthotic. (C)
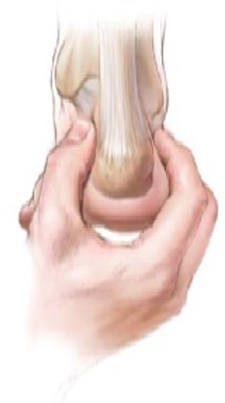
- The most distinguishing feature on physical exam is the exquisite heel pain produced by lateral and medial compression (“squeezing”) of the heel. (C)
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Two things about calcaneal “apophysitis” are a bit misleading. The first is its name. Although this common cause of heel pain in adolescents and teenagers was once considered a true osteochondritis, we now know that it’s actually a mechanical overuse pain syndrome with a self-limited, benign prognosis.1-3 The second area of confusion is what you’ll see on x-ray: an increased density and irregular fragmentation that was once viewed with suspicion, but is actually a normal pattern of ossification for this particular apophysis.
Don’t let the x-ray fool you
Primary care physicians can properly manage this common pain condition, given an understanding of the features, natural history, and treatment principles presented here.
Orthopedic referral is indicated for only a few recalcitrant cases.
Shoes aren’t to blame, but activity level is
Adolescents with calcaneal apophysitis—also known as Sever’s disease—will typically come into the office complaining of pain, often in both heels, particularly with mechanical activities such as running, jumping, and long-distance walking. Patients may walk on tiptoe to avoid the pain.4
The condition is common in both boys and girls, although personal experience indicates it’s more common in boys. The typical age of the patient is 8 to 15 years. The condition is most commonly seen in patients who are engaged in athletic endeavors,5,6 including soccer, basketball, and gymnastics,7,8 though no specific athletic endeavor has been directly implicated in the pathogenesis. Likewise, no specific foot structure or type of shoe wear has been directly related to the symptomatology.
Should Johnny quit the track team?

Exquisite heel pain produced by medial and lateral compression of the heel is the most distinguishing feature of calcaneal apophysitis
An otherwise healthy boy, age 12, walks into your office—on tiptoe. His problem is pain in both heels, especially when running. It’s his first season on his school track team, and he says he’s been practicing hard for the 50-yard dash, “my best event.” his parents express to you their concern about possible sports-related injuries or underlying disease, and their son’s distress about the possibilty of “letting down the team” if he quits. You find no swelling, no skin changes, no erythema, and no other local abnormalities. Symptoms of marked pain are produced by medial and lateral compression (squeezing) of the heel at the site where the calcaneal apophysis attaches to the main body of the os calcis. There is no pain on plantar, posterior, or retrocalcaneal pressure, or adjacent to the Achilles tendon.

Exquisite heel pain produced by medial and lateral compression of the heel is the most distinguishing feature of calcaneal apophysitis
Is this x-ray normal? You order a lateral x-ray of the calcaneus to exclude other pathology. You observe a pattern of increased density and apparent irregular fragmentation on the x-ray. The radiologist reports no abnormal findings. The above x-ray typifies calcaneal apophysitis, an overuse syndrome often seen in children 8 to 15 years of age. The “dense” area is actually a secondary ossification center of the calcaneus, not an indication of pathology.
The ossification of the calcaneus is different from that of the tarsal bones, which are each ossified from a single center. In the case of the calcaneus, a secondary center of ossification typically appears in girls by age 6, and in boys by age 8.14,15 During adolescence, a C-shaped cartilage develops between the metaphyseal bone of the body of the calcaneus and the secondary center (or centers) of ossification. Then, at around age 10 or 11, a more superior tertiary ossification center appears in the apophysis of the calcaneus.
As the calcaneal apophysis progressively ossifies, it presents as a very dense radiographic pattern in an adolescent. For years, this was thought to represent a form of osteochondritis.16 In fact, this is a normal pattern of ossification for this particular apophysis.17-22
What do you tell the patient and parents? You advise an in-shoe orthotic, no limits on physical activity, and no surgery. You explain that the pain is due to recurrent impact (overuse), and that the orthotic will “unload” the heel and permit symtoms to resolve, typically within 60 days. If asked about discomfort, you may advise anti-inflammatories and ice/heat.