Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 48-YEAR-OLD MAN went to his primary care physician for his annual physical. He told his physician that for the past few years, he had intermittent, painless rectal bleeding consisting of small amounts of blood on the toilet paper after defecation. He also mentioned that he often spontaneously awoke, very early in the morning. His past medical history was unremarkable.
The patient was born in Cuba but had lived in the United States for more than 30 years. He was divorced, lived alone, and had no children. He had traveled to Latin America—including Mexico, Brazil, and Cuba—off and on over the past 10 years. His last trip was approximately 2 years ago.
His physical exam was unremarkable. Rectal examination revealed no masses or external hemorrhoids; stool was brown and Hemoccult negative. Labs were remarkable for eosinophilia ranging from 10% to 24% over the past several years (the white blood cell count ranged from 5200 to 5900/mcL).
A subsequent colonoscopy revealed many white, thin, motile organisms dispersed throughout the colon (FIGURE 1). The organisms were most densely populated in the cecum. Of note, the patient also had nonbleeding internal hemorrhoids. An aspiration of the organisms was obtained and sent to the microbiology lab for further evaluation. Wet preparation microscopy is shown below (FIGURE 2).
FIGURE 1
Motile worms

Multiple motile worms were found on colonoscopy, dispersed throughout the colon. The worms were concentrated in the right colon.
FIGURE 2
Ova
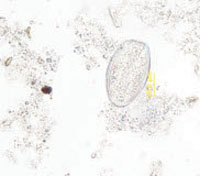
Aspiration on colonoscopy revealed football-shaped eggs that were flat on one side.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU MANAGE THIS CONDITION?