Common signs and symptoms that signal LPR
LPR is primarily a clinical diagnosis based on signs and symptoms—which are also used to rule out GERD. Notably, less than 50% of patients with LPR suffer from heartburn and regurgitation.16 Those who do have heartburn and regurgitation typically suffer with reflux during the day, when they’re in an upright position, whereas reflux associated with GERD develops primarily at night.16 The results of a recent survey of members of the American Bronchoesophagological Association highlight the most common signs and symptoms of LPR, listed below from the most to the least frequent:17
- throat clearing
- persistent cough
- globus sensation
- hoarseness
- choking episodes.
Additional signs and symptoms include excessive and chronic throat clearing, sore throat, postnasal drip, and dysphagia.
Use a validated symptom index. To further assess the probability and severity of LPR, use the Reflux Symptom Index18 (TABLE 1). A recent cohort study validated the index, with an average score of 21.2 for those with LPR, vs an average of 11.6 for controls (P<.001). A score >13 is suggestive of LPR (odds ratio=9.19), the researchers found.18
If the diagnosis remains uncertain and the patient continues to be troubled by signs and symptoms suggestive of LPR, refer him or her to an otolaryngologist for further investigation. A referral is needed, too, to rule out malignancy in any patient with 3 or more of the following red flags: older than 50 years, otalgia, weight loss, progressive hoarseness, neck mass, a significant history of alcohol use, and a history of smoking.7
TABLE 1
The Reflux Symptom Index for laryngopharyngeal reflux
| Within the last month, how did the following problems affect you? | 0 = NO PROBLEM 5 = SEVERE PROBLEM (CIRCLE THE APPROPRIATE RESPONSE) | |||||
|---|---|---|---|---|---|---|
| 1. Hoarseness or a problem with your voice | 0 | 1 | 2 | 3 | 4 | 5 |
| 2. Clearing your throat | 0 | 1 | 2 | 3 | 4 | 5 |
| 3. Excess throat mucus or postnasal drip | 0 | 1 | 2 | 3 | 4 | 5 |
| 4. Difficulty swallowing food, liquids, or pills | 0 | 1 | 2 | 3 | 4 | 5 |
| 5. Coughing after you ate or after lying down | 0 | 1 | 2 | 3 | 4 | 5 |
| 6. Breathing difficulties or choking episodes | 0 | 1 | 2 | 3 | 4 | 5 |
| 7. Troublesome or annoying cough | 0 | 1 | 2 | 3 | 4 | 5 |
| 8. Sensations of something sticking in your throat or a lump in your throat | 0 | 1 | 2 | 3 | 4 | 5 |
| 9. Heartburn, chest pain, indigestion, or stomach acid coming up | 0 | 1 | 2 | 3 | 4 | 5 |
| TOTAL SCORE= | ||||||
| *A score >13 is considered suggestive of laryngopharyngeal reflux. | ||||||
| Source: Belafsky PC et al. J Voice. 2002.18 Reprinted with permission. | ||||||
Diagnostic tools the specialists will use
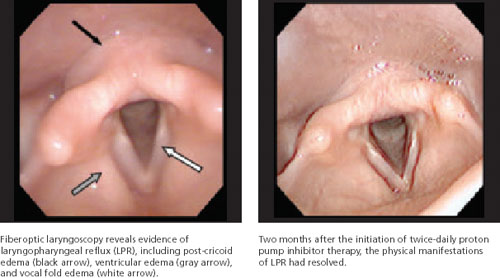
Fiberoptic laryngoscopy is the most common test used by otolaryngologists to confirm LPR and rule out other pathology. The test reveals inflammatory findings (FIGURE), such as erythema, edema, granulomas, and contact ulcers, in several anatomical locations of the larynx—especially the posterior aspect and the true vocal folds. It is important to note, however, that as many as 70% of the general population will have some laryngeal inflammation, so these findings alone are not definitive evidence of LPR.7
FIGURE
Fiberoptic laryngoscopy: Before and after treatment
Ambulatory 24-hour dual sensor pH probe monitoring is sometimes used as an adjunctive test to confirm LPR. In 2005, 2 meta-analyses found that the pH probe is reliable and sensitive and specific enough to identify significantly more acid reflux in patients with LPR than in controls.19,20 However, not everyone agrees: Some clinicians question its use as a diagnostic tool for LPR, citing problems with observer reliability, among other things. Because it increases costs to the patient and is impractical, pH monitoring is not widely used by specialists, but primarily as a research tool.21,22
Barium swallow and esophagogastroduodenoscopy (EGD) are relatively common diagnostic tools used to identify anatomical abnormalities in the gastrointestinal tract, such as a Schatzki’s ring or hiatal hernia, that can lead to symptoms of GERD and/or LPR. Some studies suggest that all patients with symptoms of LPR should undergo EGD to screen for esophageal adenocarcinoma.23,24 Because LPR symptoms are relatively common, however, many clinicians believe that EGD should be considered only when heartburn is a primary complaint in a patient with signs and symptoms of LPR—or when a patient believed to have LPR fails to respond to medical management.24
Treating LPR: Lifestyle changes, drug therapy
For all patients with LPR, dietary and lifestyle modifications have been shown to be both clinically effective and cost effective.25 In addition to dietary restrictions (TABLE 2), advise patients to avoid eating too rapidly or drinking large quantities of fluid. Late night meals—indeed, eating within 3 hours of bedtime—should also be avoided, as should heavy lunches and dinners. Tell patients to eat small, frequent meals instead.7,25,26
Recommend other behavioral changes, as well. Tell patients to avoid tight clothing, lying down immediately after a meal, and applying pressure to the abdomen, whether through exercise, heavy lifting, singing, or bending over. Smoking and overuse (or misuse) of the voice—screaming at a concert or singing for hours, for instance—are contraindicated, as well.7,25,26