Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 10-YEAR-OLD AFRICAN AMERICAN GIRL was brought to our clinic for right anterior thigh pain that she’d had for 3 weeks. She had been playing normally prior to the onset of pain and said she hadn’t experienced any trauma or injury. She was unable to run due to the pain, but continued to walk with a limp. She denied any other joint pain, fevers, rash, or other constitutional symptoms.
The patient, who was overweight and not in any distress, held her right leg in a slight external rotation. There was no asymmetry, deformity, or swelling in her right hip. She was slightly tender to palpation in the area of the right proximal anterior femur. The remainder of the right lower extremity was nontender.
The patient’s active flexion was limited to approximately 90 degrees, secondary to pain. She had marked pain with internal rotation, but none with external rotation. Her neurological exam was normal, with normal sensation throughout her right lower extremity. She had normal dorsalis pedis and posterior tibial pulses.
Plain radiographs of the right hip showed a deformity best noted on the frog leg lateral view (FIGURE 1A). The patient underwent successful in situ pinning of the right hip (FIGURE 1B), had an uncomplicated postoperative course, and returned to her prior level of activity without limitations.
Seven months later, though, the patient came back to the clinic with the same complaints—this time in her left hip—with similar x-ray findings (FIGURE 2A).
FIGURE 1
X-rays before, after pinning
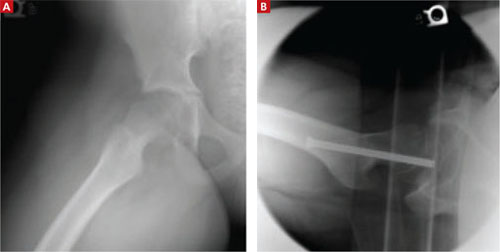
A frog leg lateral view of the patient’s right hip deformity before surgery (A). The patient underwent successful in situ pinning of the hip (B).
WHAT IS YOUR DIAGNOSIS?