Since chronic HBV infection cannot be cured, the desired clinical outcome is for patients to enter and remain in the inactive HBsAg carrier phase. Evidence suggests that, in this phase, the risk of decompensated cirrhosis may also significantly decrease.9 A few inactive HBsAg carriers (0.5%/year) will clear the surface antigen and may develop protective antibodies (anti-HBs). Development of cirrhosis after loss of HBsAg is extremely rare; however, the risk of HCC, although reduced, is not eliminated.10
If a patient is unable to suppress the virus, or if infection reactivates after the patient achieves inactive carrier status, antiviral therapy may still decrease the risk of cirrhosis and HCC through durable suppression of HBV DNA to low or undetectable levels and normalization of ALT. Seven drugs are approved by the U.S. Food and Drug Administration (FDA) for treatment of chronic hepatitis B infection (TABLE 2).3 The decision to treat must take into account multiple factors, including phase of disease, age of the patient, extent of liver involvement on biopsy, potential efficacy of and adverse events associated with available therapies, cost of long-term medication, and, importantly, the high risk of development of nucleos(t)ide analog-resistant viral strains. Many studies have demonstrated the benefit of treating patients with advanced fibrosis or cirrhosis.9,11–13 However, no study has shown a benefit of treating those in the immune tolerant or inactive carrier phases.
TABLE 1
Phases of chronic HBV infection (HBsAg+ >6 mos)6
| Phase | Labs and histology |
|---|---|
| immune tolerant | HBV DNA >20,000 IU/mL* ALT normal HBeAg detectable No or minimal liver inflammation and fibrosis |
| Immune active | HBV DNA usually >20,000 IU/mL* ALT elevated HBeAg may be detectable or not; anti-HBe may be present Liver inflammation and fibrosis can develop |
| Inactive HBsAg carrier | HBV DNA <2000 IU/mL or undetectable* ALT normal HBeAg undetectable; anti-HBe present Minimal to no liver inflammation; fibrosis may regress |
| Reactivation | HBV DNA levels increase ALT normal or elevated HBeAg undetectable. |
| ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; HBsAg, hepatitis B surface antigen; HBeAg, hepatitis B e-antigen; HBV, hepatitis B virus. *For HBV DNA: 2000 IU/ml=104 copies/ml; 20,000 IU/mL=105 copies/mL | |
TABLE 2
FDA-approved drugs for the treatment of chronic HBV infection3
| Drug | labeled for use in: |
|---|---|
| Interferons | |
| Interferon alfa-2b (Intron A) | Adults; children >12 months |
| Peginterferon alfa-2a (Pegasys) | Adults |
| Nucleos(t)ide analogs | |
| Lamivudine (Epivir-HBV) | Adults; children >3 years |
| Adefovir dipivoxil (Hepsera) | Adults; children >12 years |
| Entecavir (Baraclude) | Adults; children >16 years |
| Telbivudine (Tyzeka) | Adults |
| Tenofovir disoproxil fumarate (Viread) | Adults |
| HBV, hepatitis B virus. | |
Key opportunities to make a difference
Primary care providers can form an effective first-line of defense against morbidity and mortality associated with chronic HBV infection by:
- immunizing all infants, children, and adolescents, as well as adults at risk to acquire HBV, following guidelines from the CDC and American Academy of Pediatrics;
- screening those at high risk, as per CDC guidelines;
- performing clinical and laboratory evaluation of patients who have chronic HBV infection, to determine current phase of disease;
- monitoring patients in the immune tolerant or inactive phases every 6 to 12 months for disease progression; and
- consulting with a liver specialist or HBV-experienced provider for patients in the immune active phase, to determine treatment strategies.
Our panel has developed an algorithm (FIGURE) that addresses the screening of individuals at risk of contracting HBV and the evaluation and monitoring of those who are identified as HBsAg-positive. Although the algorithm cannot anticipate all possible clinical circumstances, it offers a general path forward based on the results of routine laboratory tests. Ideally, an office system—whether using electronic medical records or not—would incorporate guideline-based prompts for screening and management.
FIGURE
Suspect HBV infection? Use this algorithm to screen and intervene
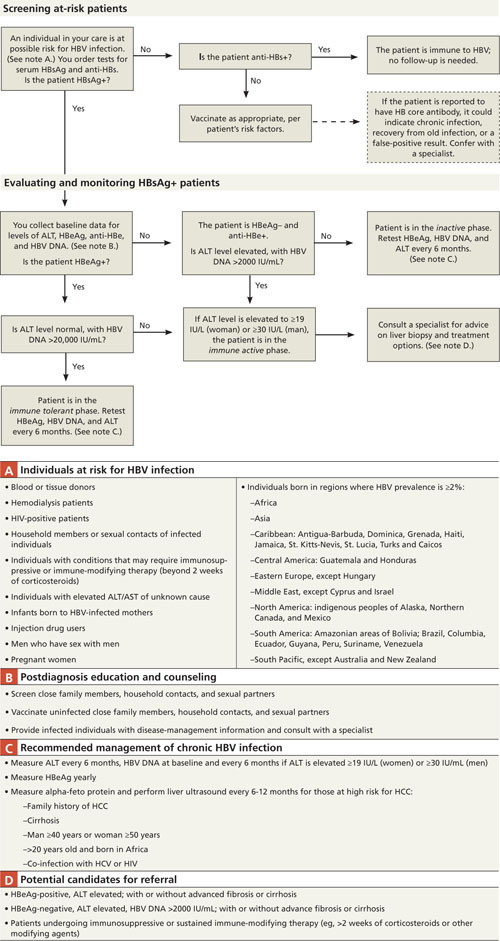
ALT, alanine aminotransferase; anti-HBe, antibody to HBeAg; anti-HBs, antibody to HBsAg; AST, aspartate aminotransferase; DNA, deoxyribose nucleic acid; HBeAg, hepatitis B e-antigen (protein produced by HBV, indicating heightened viral activity); HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HIV, human immunodeficiency virus; HCC, hepatocellular carcinoma.
Source: Primary Care Provider Workshop on Hepatitis B, sponsored by the Hepatitis B Foundation in Doylestown, Pa (March 10-11, 2010).
Underuse of screening means many infected individuals are missed
The CDC has identified high-risk groups for HBV screening, including all individuals born in geographic regions where HBsAg prevalence is ≥2% (FIGURE, NOTE A).4 Screening is simple and relatively inexpensive (commercial diagnostic laboratories currently charge $150-$250 to screen for HBsAg and anti-HBs). Despite these recommendations, the recent IOM report confirms that screening is under-used or is not being done appropriately.2
Screening is also recommended for individuals about to undergo immunosuppressive or immune-modifying therapy (eg, for treatment of cancer, rheumatoid arthritis, or inflammatory bowel disease, or in preparation for bone marrow or other transplant). For these patients who are also asymptomatic inactive carriers of HBV, the risk of reactivation can be as high as 50%, especially in patients receiving chemotherapy for lymphoma. Deaths from fulminant hepatitis have also been reported; however, preemptive HBV antiviral treatment can reduce this risk to about 10% or less.14,15 The workshop panel recommends that providers screen for HBV under these circumstances, and that HBsAg-positive patients should start preemptive oral HBV antiviral therapy before receiving immunosuppressive or immune-modifying therapy (including systemic corticosteroids >2 weeks) to prevent a flare of hepatitis.2