Facility with these roles may be a function of personal talent, introspection, and experience. The physicians studied reported that competence with these roles grew over time through delivering endof-life care and learning from patients, families, and other caregivers. Less experienced clinicians tended to describe the consultant and collaborator roles only. Clinicians describing the guide role had been in practice at least a decade and thus were at least 17 years into their training and practice in medicine. Apparently, expertise in all 3 roles requires not only excellent technical diagnostic and treatment skills but also the complex integrated skills of relational knowledge and caring gained through experience.
Our data indicate that relationship, meaning, and roles are primary moderators of the organization of exemplary end-of-life care. Yet, it appears to take nearly 2 decades for physicians to gain the confidence in their knowledge, skills, and attitudes necessary to comfortably guide patients and families through the nuances of end-of-life care. How to successfully educate clinicians to use such a model earlier is beyond our scope but appears crucial to improving training efforts. Current attempts to teach end-of-life care do not develop and explore the complex integrative domains of relational knowledge37-40 described in our study. Studies of educational interventions that stress the importance of the relational aspects of end-of-life care appear warranted.
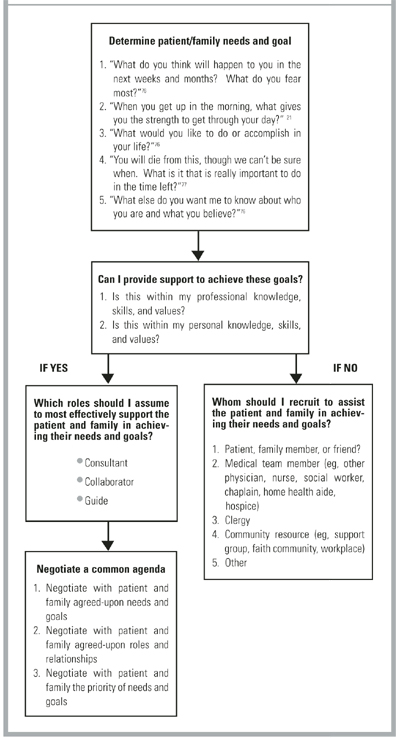
To facilitate skill acquisition, the authors propose the steps diagrammed in the Figure to assist clinicians in providing quality end-of-life care. We believe the time spent determining patient-centered goals and the roles and relationships required by the clinician should at least equal the time spent determining which tests and treatments to provide. At the end of life, when tests and treatments result in fewer benefits and greater risks and burdens, determining patient and family needs and goals becomes increasingly important as management changes from cure to care.
FIGURE
FLOW DIAGRAM FOR CLINICIAN ROLES
Limitations
This study is limited by a study sample of primary care, family practice faculty who geographically represent all practice in the Pacific Northwest and are predominantly Euro-American in ethnicity. The majority are family physicians, with the remainder pediatricians, internists, and a small number of nurse practitioners and physician assistants. Although no significant differences in terms of roles, relationships, and personal meanings between professional groups were noted, whether these findings are transferable to other primary care clinicians in community practice is unknown. Whether non–primary care specialists and clinicians of differing ethnicity or geographic region would respond differently is unknown. Generalizing these findings to non–primary care clinicians and clinicians of color requires further research.
Conclusions
Given the enormity of social and cultural values that make death a taboo topic, it is unclear how any single reform can easily overcome the multiple barriers to improved end-of-life care. Whether it is possible to teach attitudes and values, such as empathy and self-reflection, is uncertain, though promising curricula and research exist.41-42 If primary care physicians and other professionals improve their knowledge, skills, and attitudes in the delivery of such care, the ultimate effect on improving the experience of patients and families will require further study.
Acknowledgments
We wish to thank the Emily Davie and Joseph S. Kornfeld Foundation and The Nathan Cummings Foundation, New York, which provided generous grants that made our study and article possible. Additionally, we thank Phyllis Silverman, PhD, Harvard University, for her early counsel and advice; Tom Taylor, MD, PhD, University of Washington School of Medicine, for his thoughtful input into the study design, his sage guidance, and his review of the manuscript; Jeanne Quint Benoliel, DNS, Professor Emeritus, University of Washington School of Nursing, for her inspiration and review of the study design and results; and Greg Guldin, PhD, Pacific Lutheran University, for his thoughtful review of the manuscript.