- When are x-ray films indicated for a patient with knee pain?
- When should we prescribe selective cyclo-oxygenase-2 (COX-2) inhibitors, instead of nonsteroidal anti-inflammatory drugs (NSAIDs)?
- How often can intraarticular steroids be used?
- What is the role of viscosupplementation?
- When is total knee replacement appropriate?
Answers to these and other questions can be found in a guideline revised within the year by the Evidence-Based Practice Committee of the American Academy of Orthopedic Surgeons. The guideline—revised from a version developed and released in 1996—is divided into 2 phases: care provided by the first-contact primary care physician (the focus of this review), and recommendations for specialists (not addressed in this review).
The major recommendations summarized in the National Guideline Clearinghouse (www.ngc.gov) did not include the excellent care algorithm. For this update, therefore, the source document was accessed. It summarizes the following recommendations for referral to a musculoskeletal specialist (orthopedist, physiatrist, or rheumatologist)—poor response to 12 weeks of treatment, suspected infection, or hemarthrosis.
The evidence categories for this guideline are diagnosis, evaluation, management, and treatment. Targeted patients were adults with longstanding knee pain. Outcomes measured were symptomatic pain relief, improved range of motion, better physical functioning, and complications associated with treatment.
The committee used a recommendation rating scheme of A to D, based on a review of the evidence. Ratings were altered to correspond to the grades of recommendation of the Oxford Centre for Evidence-Based Medicine. (As explained on pages 111 to 120 of this issue, The journal of family practice and many other family-medicine publications will be using an evidence-rating system ranging from A to C. For this review, however, the scheme of A to D originally used by the guideline’s authors has been left intact.)
Limitations of guideline usefulness
Although this guideline was just published, the evidence is complete only through 2000. The bibliography is lengthy, but the support document does not provide evidence tables. The established outcomes set forth were not used to design the algorithm, which also lacks grades of evidence. The guideline is further weakened by the lack of cost-effectiveness analysis.
Guideline development and evidence review
The 1996 guideline was developed by a multidisciplinary group of American Academy of Orthopedic Surgeons, the American Association of Neurological Surgeons, the American College of Physical Medicine and Rehabilitation, and the American College of Rheumatology. The 2003 revision group performed a new literature search for 1990–2000 for human subjects aged 19 years and older. In all, 128 articles were reviewed, 114 references were cited, the evidence was graded, and the original guideline was revised based on the evidence.
Sources for this guideline
American Academy of Orthopaedic Surgeons. AAOS clinical practice guideline on osteoarthritis of the knee. Rosemont, Ill: American Academy of Orthopaedic Surgeons; 2003.
Source document available at: www.aaos.org/wordhtml/pdfs_r/guidelin/suprt_04.pdf. Algorithm available at: www.aaos.org/word-html/pdfs_r/guidelin/chart_oakn.pdf. Accessed on December 30, 2003.
Grade A Recommendations
- Initial treatment with NSAIDs or acetaminophen. acetaminophen is as effective as NSAIDs
- Physical therapy, including conditioning, quadriceps strengthening, and range of motion exercises should be considered for patients with osteoarthritis (confirmed by radiographs) after 4 to 6 weeks of conservative therapy.
Grade B Recommendations
- COX-2 Inhibitors should be used only for patients at risk of adverse renal and gastrointestinal effects from NSAIDs.
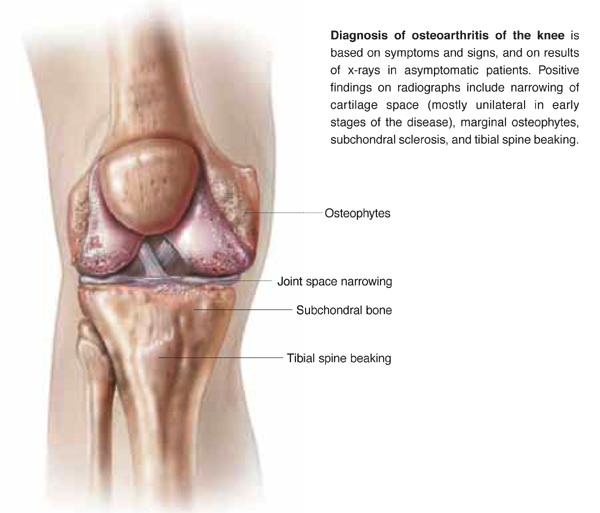
- A tangential view of the patellofemoral joint and a standing posterior-anterior view of the knee flexed 20° should be obtained for patients who do not respond to treatment in 1 to 4 weeks or whose pain returns. Positive findings are narrowing of cartilage space, marginal osteophytes, subchondral sclerosis, and tibial spine beaking.
- If the patient is unresponsive to 1 NSAID, changing to another NSAID is an option.
- Use durable medical equipment assistive devices such as canes, fitted footwear, and braces.
- Educate patients regarding weight loss, support groups, and avoidance of activities that worsen knee pain.
Grade C Recommendations
- Viscosupplementation may be effective during the first 12 weeks of symptoms.
Grade D Recommendations
- Knee x-ray for patients with persistent pain (1–4 weeks) or return of pain after a symptom-free interval.
- With long-term NSAID use, monitor complete blood count, renal functions, liver functions, and stool guiac every 6 months.
- Arthrocentesis and intra-articular steroid injection are options for persistent pain (1–4 weeks).
- Chondroitin and glucosamine have not been studied adequately to make recommendations.
FIGURE
Osteoarthritis of the knee
- Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update.American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000; 43:1905–1915. Available at: www.rheumatology.org/publications/guide-lines/oa-knee/oa-knee.asp. Accessed on December 30, 2003.
- Knee pain or swelling: acute or chronic. University of Michigan Health System. Ann Arbor, Mich: University of Michigan Health System; 2002 Aug. Available at: cme.med.umich. edu/pdf/guideline/knee.pdf.
- Diagnosis and treatment of adult degenerative joint disease (DJD) of the knee. Institute for Clinical Systems Improvement (ICSI). Bloomington, Minn: Institute for Clinical Systems Improvement (ICSI); 2002 May. Available at: www.icsi.org/knowledge/browse_ category.asp?catID=29.
- Pain in osteoarthritis, rheumatoid arthritis, and juvenile chronic arthritis. Simon LS, Lipman AG, Jacox AK, et al. 2nd ed. Glenview, Ill: American Pain Society (APS); 2002. Not available on-line.
- Physical activity in the prevention, treatment, and rehabilitation of diseases. Finnish Medical Society Duodecim. Helsinki, Finland: Duodecim Medical Publications Ltd.; 2002 May 7. Available at: www.ebm-guidelines.com/home.html (fee for access).
Correspondence
Keith B. Holten, MD, Clinton Memorial Hospital/University of Cincinnati Family Practice Residency, 825 W. Locust St., Wilmington, OH, 45177. E-mail: keholtenmd@cmhregional.com.