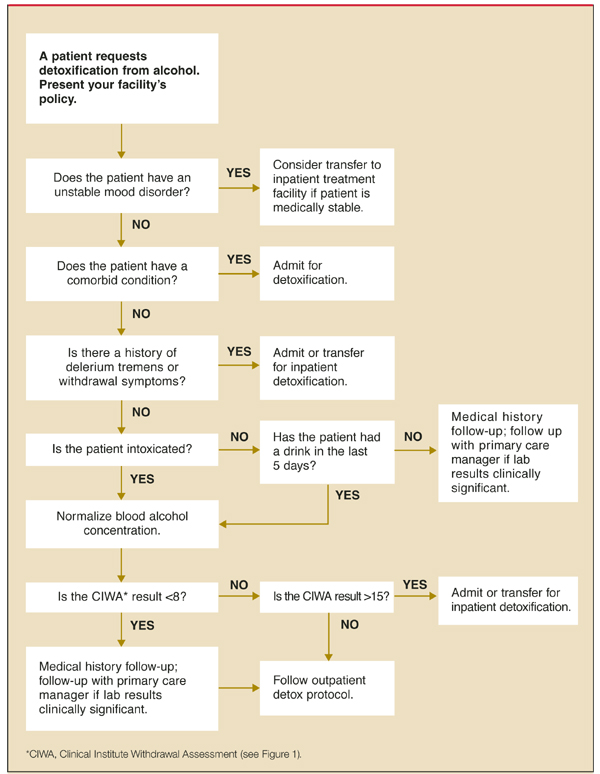
FIGURE 2
Guiding a patient through alcohol detoxification
Anticonvulsants
Attractive alternatives to benzodiazepines include the anticonvulsants carbamazepine (Tegretol) and valproic acid (Depakote).
Carbamazepine. Carbamazepine has been used successfully for many years in Europe,21 but has not been used widely in the US due to the safety, efficacy, and familiarity of benzodiazepines (Table 1). The use of anticonvulsants, however, has several advantages. They are not as sedating as benzodiazepines and do not have the abuse potential, making them particularly useful in the outpatient setting.
The use of anticonvulsant medication decreases the possibility of seizures, one of the more serious complications of alcohol withdrawal (NNT=36) (LOE: 1, 2 double-blind randomized controlled trials). The brain cell kindling-like phenomenon—in which repeated episodes of alcohol withdrawal is associated with increasing severity of withdrawal—is decreased with the anticonvulsant carbamazepine.14
In a double-blind controlled trial comparing carbamazepine with oxazepam, carbamazepine was shown to be superior in ameliorating global psychological distress and reducing aggression and anxiety.21 Stuppaeck et al showed that for alcohol withdrawal longer than 5 days, carbamazepine was statistically superior (P<.05) to oxazepam in reduction of CIWA scores.22,23 Carbamazepine is also superior to benzodiazepines in preventing rebound withdrawal symptoms and reducing post-treatment drinking, especially in those with a history of multiple repeated withdrawals (SOR=A).22 It has been shown that patients treated with carbamazepine were less likely to have a first drink following detoxification, and if they did drink, they drank less. This difference was especially evident for those patients with a history of multiple withdrawal attempts.22
A limitation of carbamazepine use, however, is its interaction with multiple medications that undergo hepatic oxidative metabolism, making it less useful in older patients or those with multiple medical problems. In summary, in generally healthy individuals with mild-to-moderate alcohol withdrawal, carbamazepine is just as efficacious as benzodiazepines, but has many advantages making it the drug of choice for properly selected patients (SOR=A).21-23
Valproic acid. Another widely used anticonvulsant, valproic acid, significantly affects the course of alcohol withdrawal and reduces the need for treatment with a benzodiazepine (LOE: 1).24 Two double-blind, randomized studies showed that patients treated with valproic acid for 4 to 7 days had fewer seizures, dropped out less frequently, had less severe withdrawal symptoms, and require less oxazepam than those treated with placebo or carbamazepine.24,25
Although effective, valproic acid use may be limited by side effects—somnolence, gastrointestinal disturbances, confusion, and tremor—that mimic the symptoms of alcohol withdrawal, making it difficult to assess improvement.
Other types of medications
Alpha-adrenergic agonists,24,30, beta-blockers,31,33 and calcium channel blockers34,35 have been used to control symptoms of acute alcohol withdrawal, but have demonstrated little efficacy in prevention of seizures or DTs (LOE: 1).5,36
Treatment regimens
The acceptable medication regimens for treating alcohol withdrawal are the gradually tapering dose approach, the fixed-schedule approach, and the symptom-triggered approach. The first 2 regimens are appropriate for the pharmacological treatment of outpatient alcohol detoxification.
Gradually tapering regimen. With the gradual-dosing plan, patients receive medication according to a predetermined dosing schedule for several days as the medication is gradually discontinued (Table 2).
Fixed-schedule regimen. In the fixed-schedule dosing regimen, the patient receives a fixed dose of medication every 6 hours for 2 to 3 days regardless of severity of symptoms.
Symptom-triggered regimen. For the symptom-triggered approach, the patient’s CIWA-Ar score is determined hourly or bihourly and the medication is administered only when the score is elevated. Typically, benzodiazepines are used in a symptom-triggered regimen, although either benzodiazepines or anticonvulsants may be used in a fixed-schedule plan.
The main advantage to the symptom-triggered approach is that much less medication is used to achieve the same withdrawal state (LOE: 1).37-39 The symptom-triggered approach has also shown a possible decrease in DTs and may lead to less oversedation.38,39
We favor a symptom-based approach whenever adequate periodic assessment of CIWA-Ar can be performed, such as in an inpatient setting. For those patients who require pharmacological treatment during outpatient detoxification (CIWA-Ar score 8–15), we prefer the gradually tapering or fixed dosing plan, to provide a margin of safety, simplify the dosing schedule, and maximize compliance (SOR: C, expert opinion).14
TABLE 2
Outpatient treatment for alcohol detoxification
| Thiamine – 100 mg orally per day (for 5 days) |
| Consider folate (1 mg) and multiple vitamin injection |
| One of the following regimens: |
| 3-day supply (only) of the following: Chlordiazepoxide |
| 50–100 mg every 6 hours for 4 doses, then |
| 25–50 mg every 6 hours for 8 doses |
| Diazepam |
| 10–20 mg every 6 hours for 4 doses, then |
| 5–10 mg every 6 hours for 8 doses |
| Lorazepam |
| 2–4 mg every 6 hours for 4 doses, then |
| 1–2 mg every 6 hours for 8 doses (consider this choice if significant hepatic dysfunction) |
| Carbamazepine (Tegretol) —5-day supply |
| 200 mg 4 times on day 1, |
| 200 mg 3 times on day 2, |
| 200 mg 2 times on day 3, |
| 200 mg daily for 2 more days (5 days total) |