Discussion
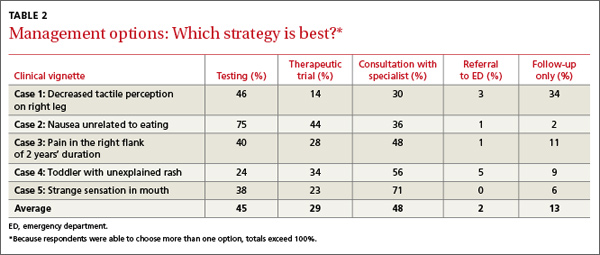
Patients with undiagnosed signs and/or symptoms present a significant challenge in primary care. In such cases, physicians prefer a work-up to follow-up, with a confidence level in their management strategy that is higher than for their diagnostic hypotheses. There appears to be a stronger perceived need to “do something” than to engage in watchful waiting and follow-up.
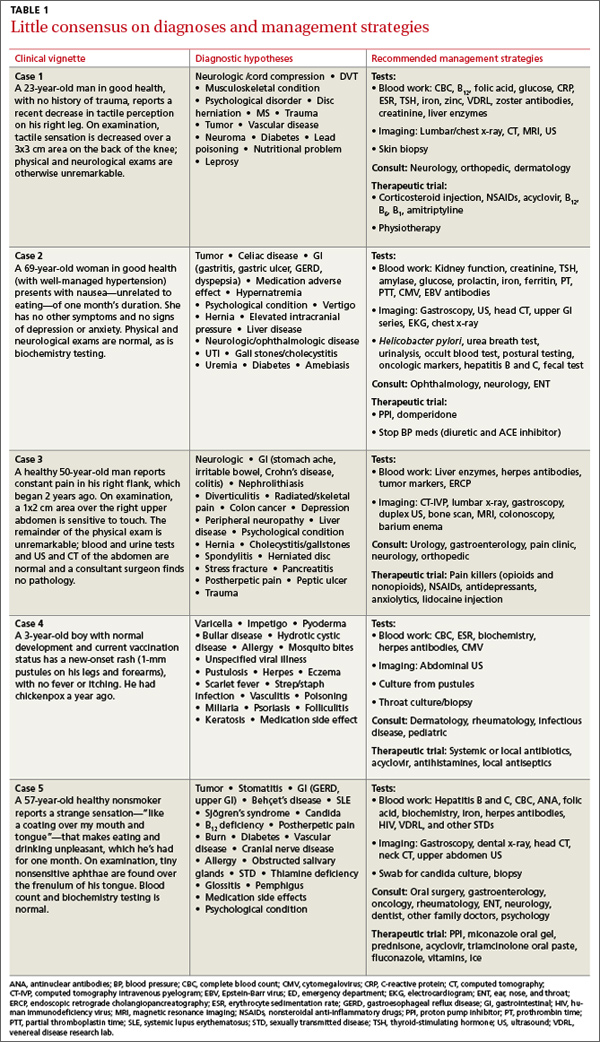
Symptoms subside without treatment. Notably, in all the cases that formed the basis for the clinical vignettes used in our survey, the patients’ complaints eventually subsided, with no specific therapy. In some cases of unclear diagnosis, an active work-up may be justified; in others, watchful waiting before testing for unexplained complaints may be preferable.
Action bias. The preference for action over inaction in all the cases presented suggests what has been described as “action bias.”9 The term is derived from sports; in soccer penalty kicks, for example, it applies to goalkeepers who jump before they can see the kick direction and miss.10 According to the norm theory,11 such errors of commission derive from players’ perception that they are expected to act.10 Conversely, in instances in which inaction is the norm, an omission bias prevails, as people tend to judge acts that are harmful as worse than omissions that are even more harmful.10 In medicine, action bias has been found to influence clinical practice and contribute to overuse of both diagnostic testing and procedures.12-14
Gender difference. Gender has been shown to affect self-perception in cognitive bias.15 In a study of confidence levels among undergraduate students, overconfidence was found to be more prevalent among males than females, particularly for incorrect answers.16 This observation may relate to the gender differences in our study in physicians facing diagnostic uncertainty.
Study limitations. Our research was limited by the nature and type of our sample, but because the inclination to act was found in both immigrant and native practitioners, the observation of action bias could be generalizable to all primary care physicians. The clinical vignettes we chose may not be representative of commonly seen cases of medically unexplained symptoms. Also, our questionnaire was not tested beyond at face validity. It is possible, too, that nonresponders would be less inclined to action in the face of uncertainty. With the high (77%) response rate to our survey, however, their inclusion would be unlikely to strikingly alter the results.
Another limitation inherent to the design of our study is that physicians may respond to vignettes in a way that is substantially different than their response in actual practice. In a practice setting, physicians are able to listen to a full narrative and apply various doctor-patient communication tools, which are especially important in the context of unexplained complaints.17 On the other hand, the artificial setting may reduce the fear of litigation. Our observation of greater confidence in the need for action than for the diagnostic hypothesis is consistent with testing overuse in field studies.6 The fact that our survey went only to physicians affiliated with academic centers is another potential limitation, although it is not clear whether these clinicians differ from nonacademic physicians in their approach to unexplained complaints. Finally, the design of this study did not allow us to explore the reasons for action bias, a task that might be addressed in focus groups or interviews.
A closer look at bias. Our findings suggest a need for more in-depth research on potential biases that drive medical overuse, as part of an overall strategy to improve physicians’approach to medically unexplained symptoms.17 Remedies may require training, practice and failure feedback, quality improvement tools, and innovative management strategies.1,18 Uncertain diagnosis appears to be a frequent challenge in primary care settings. Inthe face of uncertainty, weighing the potential harms of overtesting vs follow-up and facilitating an informed decision-making process with the patient may lead to a reduction inaction bias,19 and thus, in the increased testing and higher health care consumption that often result.
CORRESPONDENCE
Mayer Brezis, MD, Center for Clinical Quality & Safety, Hadassah-Hebrew University Medical Center, 91120 Jerusalem, Israel; brezis@mail.huji.ac.il
ACKNOWLEDGEMENT
The authors thank Steven R. Simon, MD, MPH, for his help with the preparation of this manuscript.