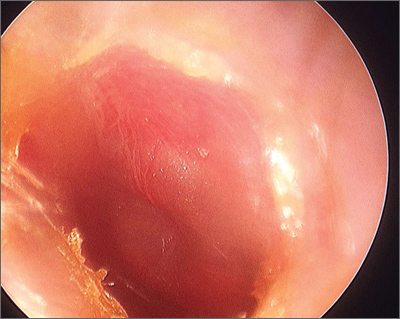
The FP diagnosed acute otitis media (AOM) in this patient. AOM is characterized by middle-ear effusion in a patient with signs and symptoms of acute illness (eg, fever, irritability, otalgia).
Oral acetaminophen and ibuprofen may reduce earache when given with antibiotics. Antibiotics seem to be most beneficial in children younger than 2 years of age with bilateral AOM, high fever, or vomiting, and in children with both AOM and otorrhea. For most other children with mild disease, an observational policy is acceptable.
Antibiotics may lead to more rapid reduction in symptoms of AOM, but increase the risk of adverse effects including diarrhea, vomiting, and rash. Antibiotics seem to reduce pain at 2 to 7 days, and may prevent development of contralateral AOM, but increase the risk of adverse effects compared with placebo. Antibiotics found to be effective in AOM include amoxicillin, amoxicillin/clavulanic acid, ampicillin, penicillin, erythromycin, azithromycin, trimethoprim-sulfamethoxazole, and cephalosporins. Amoxicillin is a good first-line treatment because it is inexpensive and children tolerate the bubblegum taste well.
Longer (8- to 10-day) courses of antibiotics reduce short-term treatment failure but have no long-term benefits compared with shorter regimens (5-day courses). An observational approach substantially reduces the unnecessary use of antibiotics in children with AOM and may be an alternative to routinely treating them with antimicrobials.
In this case, the FP prescribed a 10-day course of amoxicillin and the child recovered uneventfully.
Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. Photo courtesy of William Clark, MD. This case was adapted from: Rayala B. Otitis media: acute otitis and otitis media with effusion. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:170-179.
To learn more about the Color Atlas of Family Medicine, see: http://www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/ref=dp_ob_title_bk
You can now get the second edition of the Color Atlas of Family Medicine as an app for mobile devices by clicking this link: http://usatinemedia.com/