It is important to note, however, that only one of the individual components of the primary endpoint—unstable angina—was significantly reduced by EPA (2.1% vs 1.6%; P=.014).8 In the Alpha Omega trial,9 various n-3 polyunsaturated fatty acids were tested in combination with statins. None was found to be superior to placebo in reducing cardiovascular outcomes.
Based on the evidence, the new cholesterol guideline does not support the routine use of these agents to reduce atherosclerotic CVD (See “The new cholesterol guideline: Beyond the headlines”.)11
Statins and kidney disease: Factors to consider
More than half of the deaths in patients with end-stage renal disease (ESRD) are from cardiovascular causes.12 The relationship between renal dysfunction and cardiovascular events is independent of other risk factors, including a history of CVD. Risk rises with an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73m2, with a sharp increase when the rate <45 mL/min/1.73m.2 Thus, strategies known to reduce major cardiovascular events in the general population, including statins, have the potential to offer substantial benefit for patients with chronic kidney disease (CKD).
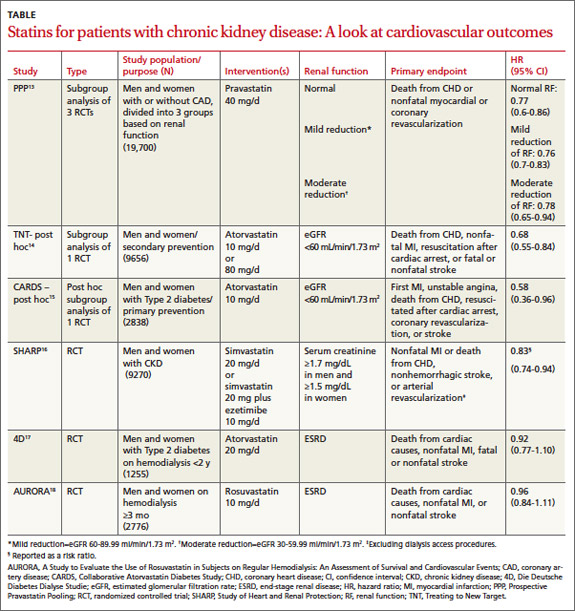
Statin use in patients with CKD has been evaluated in post-hoc and subgroup analyses of large clinical trials and, more recently, in RCTs targeting patients with both moderate and end-stage disease (TABLE).13-18
Three post-hoc analyses of large multicenter, double-blind RCTs13-15,19 compared patients with normal renal function with those with CKD. All 3 found that moderate or high-intensity statin therapy significantly reduced the incidence of the primary outcome—a composite of major cardiovascular events—compared with either placebo or a lower-intensity statin.
For patients with CKD, drug combo lowered the risk
The SHARP trial17 (N=9270) was the first large prospective, double-blind, multicenter RCT to compare the effect of a statin plus a second lipid-lowering drug (simvastatin plus ezetimibe) vs placebo in patients with CKD. A third of the participants were on dialysis at the start of the trial (ESRD was defined as starting long-term dialysis or requiring kidney transplantation).
Patients in the intervention group were significantly (17%) less likely to experience a major atherosclerotic event compared with those on placebo. This translated into an NNT of 47 over a period of 4.9 years. (Since no group received only simvastatin, it is not known what role ezetimibe had in the reduction of cardiovascular events.) Although no difference in outcomes was found when the results were stratified based on whether participants were on dialysis, this trial was not adequately powered for this subgroup analysis.17
Little benefit from statins in patients with end-stage disease
Two major prospective randomized, double-blinded, placebo-controlled, multicenter trials evaluating the effects of statin use on cardiovascular outcomes in ESRD patients on dialysis have been published.18,19 Both found a significant decline in LDL-C in patients receiving statin therapy. But neither found a significant difference in mortality rates in the statin vs placebo groups.
One group of researchers speculated that the lack of effect may be due to a difference in the pathogenesis of vascular events in patients with and without ESRD. Delayed use of statins until patients have ESRD will offer limited benefit, they concluded, and recommended against routine statin treatment in an attempt to reduce the incidence of CVD in this patient population.18 Based on these results, the new cholesterol guideline indicates that this group of patients may not benefit from statin therapy.
For patients with heart failure, statins offer limited benefit
More than half of the heart failure (HF) in the United States is caused by ischemic heart disease.20 Improvements in post-MI survival have increased the prevalence of chronic HF.
Statins have a well-established role in the prevention and treatment of atherosclerosis because of their ability to modify the natural course of the disease and reduce major adverse cardiovascular events. Thus, it seems reasonable to assume that, in patients who have or are at high risk for coronary heart disease, statins would help to prevent the occurrence or slow the progression of HF.
Early studies of statins either excluded patients with HF or enrolled so few HF patients that no conclusions could be reached regarding the safety or efficacy of statin use in this population.21-25 More recently, 2 large RCTs have studied the effect of statins in patients with HF. Both have found them to be ineffective.26,27
The CORONA trial enrolled elderly patients with HF of ischemic causes and ejection fraction ≤40% (≤35% in patients with New York Heart Association [NYHA] Class II), randomized to either rosuvastatin 10 mg/d or placebo.25 More than 40% of the participants had a history of MI, and more than 60% were NYHA Class III or IV. HF medications were well-managed; more than 90% of the patients were being treated with angiotensin-converting enzyme inhibitors or angiotensin receptor blockers; 75%, with beta-blockers; and 39%, with aldosterone antagonists.