PRACTICE RECOMMENDATIONS
› Consider novel oral anticoagualants (NOACs) for patients who have normal renal function, are comlpiant with medication regimens, and have no history of peptic ulcer or gastrointestinal bleeding. B
› Avoid overlapping warfarin with rivaroxaban or apixaban when transitioning a patient from one anticoagulant to the other, as both agents prolong prothrombin time. B
› When initiating a NOAC, it is not necessary to overlap with a parenteral anticoagulant. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Sally J is a 72-year-old Caucasian woman who comes to your clinic after being diagnosed with atrial fibrillation (AF). The patient has a 10-year history of type 2 diabetes; she also has a history of hypertension and chronic kidney disease (CKD), with a baseline creatinine clearance of approximately 40 mL/min. Ms. J tells you she knows people who take warfarin and really dislike it. She asks for your opinion of the new anticoagulants she’s seen advertised on TV, and wonders whether one of them would be right for her.
CASE 2 Bobby W, a 35-year-old African American man, was recently diagnosed with deep vein thrombosis (DVT). This was his second clot in 5 years, and occurred after a long flight home from Europe. The patient explains that he leads a very active lifestyle and doesn’t have the time to come in for the monthly international normalized ratio (INR) checks that warfarin requires. What would you recommend for these patients?
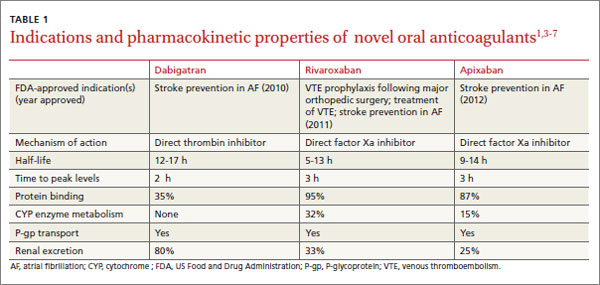
Troubled by warfarin’s narrow therapeutic index, numerous medication and dietary interactions, and need for frequent monitoring, patients requiring long-term oral anticoagulation therapy have been seeking alternatives for years. Finally, they have a choice. The US Food and Drug Administration (FDA) approved 3 oral anticoagulants—dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis)—in less than 4 years. Known as novel oral anticoagulants (NOACs), they are the first such drugs to enter the market in more than 50 years.1,2
While warfarin inhibits a wide range of clotting factors (including II, VII, IX, and X), NOACs work further down the clotting cascade (TABLE 1).1,3-7 Dabigatran, a direct thrombin inhibitor, only inhibits factor IIa.3,5 Rivaroxaban and apixaban directly inhibit factor Xa and indirectly inhibit factor IIa.3,6,7
There are notable advantages to these newer agents, but some disadvantages that must be considered, as well. Appropriate patient selection, guided by a thorough understanding of the benefits and risks of NOACs, is key.
Stroke prevention in atrial fibrillation
All 3 NOACs are approved for stroke prevention in patients with nonvalvular atrial fibrillation (AF). The approvals are based on a small number of well-designed trials: RE-LY (dabigatran), ROCKET-AF (rivaroxaban), and ARISTOTLE (apixaban).8-10 Compared with warfarin, dabigatran is the only oral anticoagulant with a lower rate of both hemorrhagic and ischemic stroke.8 Both rivaroxaban and apixaban were found to decrease overall stroke risk relative to warfarin, but the difference was driven by a lower risk for hemorrhagic, not ischemic, stroke.9,10
In these trials, overall rates of major bleeding were similar to that of warfarin.8-10 Patients taking warfarin generally experienced higher rates of intracranial hemorrhage but lower rates of gastrointestinal (GI) bleeding than those on NOACs. Relative to warfarin, apixaban was the only NOAC that did not have a higher rate of GI bleeding and the only one with a lower rate of major bleeding.8-10 In addition, apixaban remains the only NOAC found to have a statistically significant decrease in all-cause mortality compared with warfarin.10 Although dabigatran and rivaroxaban were associated with a strong trend towards decreased mortality, both studies were underpowered for this secondary outcome.8,9
Adding NOACs to stroke guidelines. The role of NOACs in the prevention of stroke in patients with nonvalvular AF is beginning to be reflected in newer guidelines. The American College of Chest Physicians (ACCP)’s 2012 guidelines recommend dabigatran over warfarin (grade 2B—weak recommendation; moderate quality evidence) unless the patient is well controlled on warfarin.11 The European Society of Cardiology (ESC)’s 2012 guidelines recommend dabigatran, apixaban, and rivaroxaban as broadly preferable to warfarin, while noting that experience with these agents is limited and appropriate patient selection is important.12
Anticoagulation to treat—and prevent—VTE
The standard of care for acute venous thromboembolism (VTE) is to initiate warfarin along with a parenteral anticoagulant, such as unfractionated heparin, low-molecular-weight heparin (LMWH), or fondaparinux.13 Due to warfarin’s slow onset to peak effect, a parenteral anticoagulant is overlapped for ≥5 days—until warfarin reaches a therapeutic level and can be continued as monotherapy.13 But many patients find subcutaneous delivery of LMWH disagreeable and costly and frequent INR monitoring inconvenient, so the new agents offer notable advantages.