PRACTICE RECOMMENDATIONS
› Advise patients to wear earplugs or earmuffs to prevent hearing loss and tinnitus when exposed to excessively loud sounds (>80dB). C
› Avoid prescribing benzodiazepines, antidepressants, or gabapentin for the treatment of tinnitus; little evidence supports routine use of these agents. B
› Consider referring patients for cognitive-behavioral therapy or tinnitus retraining therapy, each of which can reduce the bothersome nature of tinnitus. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 › Mr. L is a 47-year-old construction worker who comes to the clinic with a 3-month history of bothersome, constant, high-pitched ringing in his ears that is worse on his right side. He also reports mild hearing loss. Mr. L notes that he keeps a busy schedule, working weekends at a local shooting range. He is a 30-pack-year smoker and takes sumatriptan and nasal fluticasone spray as needed for migraines and allergies. On inspection, his ears appear normal.
CASE 2 › Ms. B, age 68 years, seeks treatment for a constant pulsatile noise in her left ear, which has been bothering her for the past 5 months. She lives alone and says this noise is worse when the house is quiet. She takes chlorthalidone for hypertension and prophylactic aspirin. She indicates that she has no problems with her hearing. On exam, the noise synchronizes with her pulse.
If Mr. L and Ms. B were your patients, what would your next steps be?
An estimated 50 million people in the United States experience some form of tinnitus,1 and the incidence is on the rise, which some have attributed to the increased use of personal music devices.2,3 Patients often describe tinnitus as a ringing noise, but it also can be perceived as buzzing, chirping, hissing, whistling, humming, or other sound. It is more often bilateral than unilateral4 and more often intermittent than continuous.1
Tinnitus may be present in childhood, but the prevalence increases with age. Surveys show that approximately 25% of adults experience symptoms and one-fourth of these patients report that it interferes with daily activities.1,2 The prevalence peaks at 31% in patients between the ages of 60 and 69 years.1
The severity of the condition ranges from causing patients to merely be aware of the noise to having substantial adverse effects on their quality of life. Because not all patients will report tinnitus symptoms, it is important to be aware of risk factors, which include advanced age, male sex, history of military service, and a work history that includes exposure to loud noise.1,2 Smoking and hypertension also are associated with higher rates of tinnitus, as is living in the southern United States.1
A subjective, or objective case of tinnitus?
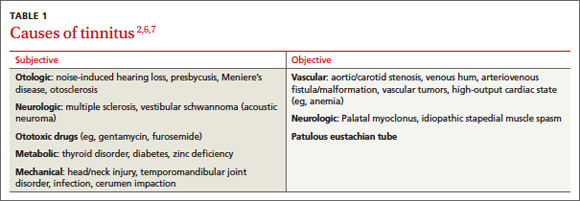
While subjective tinnitus consists of noises only the patient can hear, objective tinnitus refers to noises, including somatosounds such as turbulent blood flow or palatal myoclonus, that a physician could at least theoretically detect by auscultation or with an amplifying device. Objective tinnitus is less common than subjective tinnitus and more often has an identifiable and correctable source,5 though it may herald a serious underlying condition. When tinnitus is pulsatile or rhythmic, it may be the result of an arteriovenous fistula, arteriovenous malformation, cerebral aneurysm, arterial bruit, or other vascular lesion, such as a glomus tumor.6 Nonvascular conditions like palatal myoclonus present with clicking or low-pitched buzzing and may be a result of multiple sclerosis.7
The causes of both subjective and objective tinnitus are detailed in TABLE 1.2,6,7
Tinnitus and hearing loss: The connection
Most tinnitus is associated with hearing loss and probably results from a disruption in the normal suppression of neuronal activity in the central nervous system.2,8
Conductive hearing loss can be caused by cerumen impaction, otosclerosis, or cholesteatoma. Sensorineural hearing loss (SNHL), which is more common than conductive hearing loss, often is irreversible. The damage typically occurs in the stereocilia cells of the cochlea. These cells trigger the release of neurotransmitters that activate the eighth cranial nerve and cause abnormal excitation along the auditory pathway, giving the perception of sound in a quiet environment.2
Patients with SNHL usually have a history of prolonged exposure to loud noise (eg, heavy machinery, firearms, personal musical devices such as an iPod, or musical instruments) and often describe their tinnitus as a bilateral, high-pitched, continuous ringing. The other major category of SNHL that causes tinnitus is presbycusis—the hearing loss associated with aging—which has clinical features similar to noise-induced hearing loss.8