Providers exhibited statistically significant improvement of attitude for role adequacy (item 5), role support (item 6), job satisfaction/role-related self-esteem (item 9), and access to EMR-specific tools (items 10-12) (TABLE 2). In addition, the knowledge test score increased by 15% (P<.05) in the postintervention survey.
Staff surveys showed statistically significant improvement of attitude for job satisfaction/role-related self-esteem. There was no improvement in knowledge for staff, which is likely due to variability in training.
DISCUSSION
More than 40% of opioid prescriptions in the United States are written by primary care physicians.14 Therefore, interventions that enhance provider knowledge, institute best practices, and support role-related self-esteem in opioid management are vital to our profession.
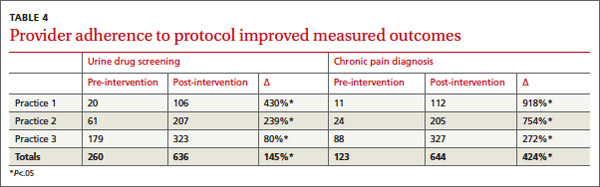
Through a straightforward protocol, we greatly increased the number of UDSs ordered (145%) and documentation of chronic pain on the problem list (424%). By increasing adherence to best practice standards, we believe this protocol will lead to improved management of patients with CNCP by providing objective urine data to guide a treatment plan, patient education with the CMA, and a documented evaluation and care plan.
In addition to fostering adherence to the protocol, our multicomponent intervention resulted in marked improvement of provider and staff attitudes toward patients taking opioids for CNCP (TABLE 2). Participants’ satisfaction in working with these patients improved significantly (27%), as did their confidence in knowing whom to ask for help with management (43%). After this intervention, physicians reported a nonstatistically significant but large reductions in the perception that patients on opioids create stress for the office (-20%), and that patients on opioids make their job harder (-18%). Knowledge about chronic opioid prescribing also improved significantly for providers (15%).
At all practices, the number of patients receiving opioids decreased, likely due to the protocol intervention.
Previous studies have shown low adoption of best practices in opioid management without a structured intervention.10 Our findings suggest that a multicomponent quality improvement intervention that combines education, financial incentive, and a structured protocol can positively impact provider and staff attitudes and adherence to best practices in caring for patients with CNCP taking opioid medications. We believe that similar interventions could be adapted by other primary care clinics with a comparable favorable impact on physician behavior, attitudes, and knowledge.
Limitations
Our findings may not apply to nonacademic practices, as we required training and the use of an EMR. Additionally, our urban patient populations may not be generalizable to rural, suburban, or other populations in the management of patients taking prescription opioids. Further, the monetary incentive, which was included in a yearly incentive package at our institution, may not be feasible at other sites.
We did not design this study to allow for practice-level comparisons or to assess patient level variables. Analysis of patient data on safety, aberrant behavior, abnormal UDS results, and the impact of the intervention on these outcomes was outside of the scope of this study. We were unable to determine whether physician turnover, particularly high in one practice, could be linked to the results.
Providers often neglected to indicate their level of training on surveys, and we were therefore unable to compare adherence and knowledge between residents and attending physicians. Additionally, we lacked approval to search individual charts to completely investigate the components of our protocol (for example, completion of a CMA or UDS). Lastly, we did not design the study to control for confounders on a provider level (such as age, gender, and years of experience). A more comprehensive review of these important variables is warranted to assess the degree to which division- or practice-level quality improvement interventions can affect provider and patient behavior change and enhance patient safety.
CORRESPONDENCE
Robin E. Canada, MD, Medical Arts Building, Suite 102, 38th and Market Sts, Philadelphia, PA 19104; robin.canada@uphs.upenn.edu
Acknowledgement
The authors gratefully acknowledge Judy Shea, PhD and Joanna Starrels, MD, who provided valuable comments in the development of this manuscript.