Danielle Snyderman, MD Brooke Salzman, MD Geoffrey Mills, MD, PhD Lauren Hersh, MD Susan Parks, MD Department of Family and Community Medicine, Jefferson University, Philadelphia, Pa danielle.snyderman@jefferson.edu
The authors reported no potential conflict of interest relevant to this article.
The risk assessment tools, medication reconciliation steps, and discharge script provided here can help you keep your patients from going back into the hospital.
› Use risk stratification methods such as the Probability of Repeated Admission (Pra) or the LACE index to identify patients at high risk for readmission. B › Take steps to ensure that follow-up appointments are made within the first one to 2 weeks of discharge, depending on the patient’s risk of readmission. C › Reconcile preadmission and postdischarge medications to identify discrepancies and possible interactions. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence B Inconsistent or limited-quality patient-oriented evidence C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Charles T, age 74, has a 3-year history of myocardial infarction (MI) and congestive heart failure (CHF) and a 10-year his-tory of type 2 diabetes with retinopathy. You have cared for him in the outpatient setting for 8 years. You are notified that he is in the emergency department (ED) and being admitted to the hospital, again. This is his third ED visit in the past 3 months; he was hospitalized for 6 days during his last admission 3 weeks ago.
What should you do with this information? How can you best communicate with the admitting team?
Hospital readmissions are widespread, costly, and often avoidable. Nearly 20% of Medicare beneficiaries discharged from hospitals are rehospitalized within 30 days, and 34% are rehospitalized within 90 days. 1 For patients with conditions like CHF, the rate of readmission within 30 days approaches 25%. 2 The estimated cost to Medicare for unplanned rehospitalizations in 2004 was $17.4 billion. 1 The Centers for Medicare and Medicaid Services penalizes hospitals for high rates of readmission within 30 days of discharge for patients with CHF, MI, and pneumonia.
Listen to Dr. Geoffrey Mills' audiocast, Learn how to get reimbursed for postdischarge care “Avoidable” hospitalizations are those that may be prevented by effective outpatient management and improved care coordination. Although efforts to reduce readmissions have focused on improving the discharge process, family physicians (FPs) can play a central role in reducing readmissions. This article describes key approaches that FPs can take to address this important issue. Because patients ages ≥65 years consistently have the highest rate of hospital readmissions, 1 we will focus on this population.
Multiple complex factors are associated with hospital readmissions
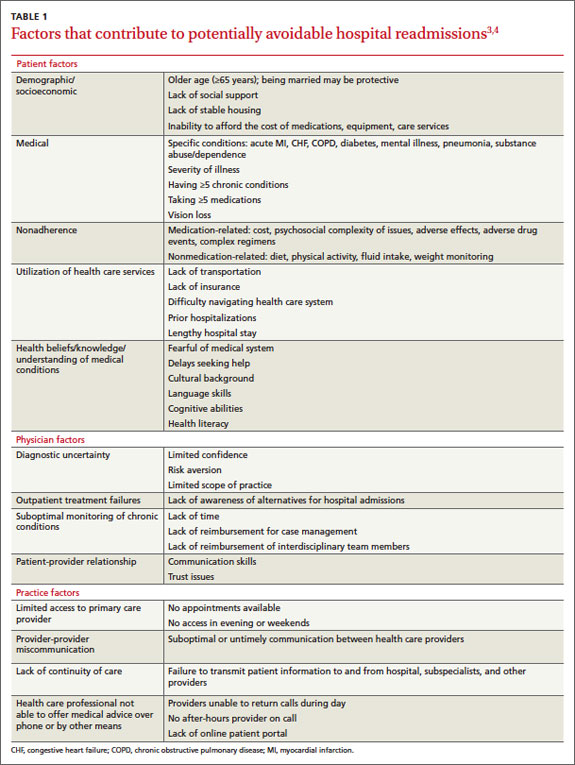
Characteristics of the patient, physician, and health care setting contribute to potentially avoidable readmissions ( TABLE 1 ).3,4
Medical conditions and comorbidities associated with high rates of rehospitalization include CHF, acute MI, pneumonia, diabetes, and chronic obstructive pulmonary disease. However, a recent study found that a diverse range of conditions, frequently differing from the index cause of hospitalization, were responsible for 30-day readmissions of Medicare patients. 5
Use a risk stratification method that captures the issues most likely to cause readmissions in your patient population, or consider using a variety of methods. Identifying those at high risk: Why and how
Determining which patients are at highest risk for readmission enables health care teams to match the intensity of interventions to the individual’s likelihood of readmission. However, current readmission risk prediction models remain a work in progress6 and few models have been tested in the outpatient setting. Despite numerous limitations, it’s still important to focus resources more efficiently. Thus, we recommend using risk stratification tools to identify patients at high risk for readmission.