› Reserve serologic testing for parvovirus B19 for pregnant women with known exposure to the virus, immunocompromised individuals, or patients with chronic hemolytic conditions or severe or persistent arthropathy. B › Keep in mind that up to 15% of children infected with human herpes virus 6 can experience febrile seizures. Treat with an antiepileptic drug, as you would for any febrile seizure that lasts >5 minutes. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence B Inconsistent or limited-quality patient-oriented evidence C Consensus, usual practice, opinion, disease-oriented evidence, case series
Fifth and sixth diseases are frequently encountered viral exanthems in family medicine. This article delineates the unique clinical characteristics of these disorders, describes rare but serious sequelae of each, and offers recommendations to guide your practice.
Fifth disease
Parvovirus B19, an infectious agent found worldwide, is the cause of fifth disease, also known as slapped cheek syndrome or erythema infectiosum. It is transmitted via respiratory droplets, most commonly in late winter and early spring. The peak incidence of parvovirus B19 infection is in children ages 5 to 15 years.1 Approximately 20% of parvovirus B19 infections remain subclinical.1,2 An observational study of children in the United Kingdom who were 6 months to 16 years of age and had been immunized for measles and rubella revealed that parvovirus B19 was the number one identifiable cause of febrile rash, responsible for 17% of cases.3 Seroprevalence increases with age, and 40% to 60% of adults test positive for prior infection.1
Clinical presentation: Not necessarily limited to fever and rash
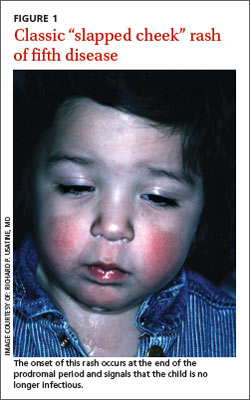
Parvovirus B19 has an incubation period of 4 to 21 days before the classic symptoms of malaise, fever, and red “slapped” cheeks appear (FIGURE 1). Four to 14 days after the onset of symptoms, a pruritic lacy rash covers the entire body, preferentially on the extensor surfaces (sparing the palms and soles), and may wax and wane for up to 3 weeks, with flaring triggered by stress, exercise, heat, or exposure to sunlight.1,4 Rarely, and usually among young adults, parvovirus B19 can cause papular-purpuric “gloves and stocking” syndrome, with fever, painful edema, erythema, and pruritus of the distal extremities.5
Associated arthritis. Parvovirus B19 may also cause a symmetric polyarthritis of the hands, wrists, knees, or ankles, particularly in adult females. The course of arthritis usually lasts 1 to 3 weeks, but up to 20% may evolve into a chronic arthritis.6 In addition, numerous case studies suggest that parvovirus B19 may, in rare cases, cause a viral myocarditis in infants and children.7
Hemolytic complications. The target of parvovirus B19 is the erythroid blood cell line.1 Consequently, immunocompromised patients and those with chronic hemolytic conditions (eg, sickle cell disease, thalassemia, spherocytosis, or pyruvate kinase deficiency) may develop hematologic complications such as aplastic crisis, chronic anemia, thrombocytopenia, neutropenia, or pancytopenia. Patients with hemolytic complications can be quite ill, presenting with fever, malaise, tachycardia, tachypnea, and profound anemia.
Parvovirus B19 may cause a symmetric polyarthritis, particularly in adult females, usually lasting one to 3 weeks. But it can evolve into a chronic arthritis.Perinatal perils. Approximately one-third of pregnant mothers are at risk for parvovirus B19 infection, and having children at home, a severe medical condition, or stressful employment have been shown to increase their risk of active infection.8 The annual incidence of symptomatic parvovirus B19 during pregnancy is 1.5%, increasing to 13% during epidemics.9 Such infection can cause significant morbidity and mortality for the fetus. Mothers newly infected during the first trimester have experienced a 71% increased risk of intrauterine fetal demise (fetal loss <20 weeks gestation) when compared with baseline risk of fetal loss.9 In one prospective observational study, fetal death was only observed when mothers were infected prior to 20 weeks of gestation.10 Intrauterine B19 infection during any trimester carries a 4% overall risk of hydrops fetalis, thought to be due to high output cardiac failure secondary to severe anemia.10
Rely on clinical findings to diagnose; restrict serologic testing
The characteristic “slapped cheek” rash usually distinguishes fifth disease from other causes of febrile rash. Differential diagnosis includes measles, scarlet fever, roseola infantum, enterovirus, and adenovirus. A diagnostic tool (TABLE) can help differentiate fifth disease from other viral exanthems.
In most cases of suspected parvovirus B19 infection, serologic testing is not indicated. However, consider serologic testing for pregnant women with known exposure to the virus, immunocompromised patients, patients with chronic hemolytic conditions, or patients with severe or persistent arthropathy. Serum immunoglobulin M can usually be detected 10 days after infection and can persist for 3 months, while serum immunoglobulin G is produced 2 weeks after inoculation and presumably lasts for life.11