Roger Zoorob, MD, MPH, FAAFP Sangita Chakrabarty, MD, MSPH, FACOEM Heather O’Hara, MD, MSPH Courtney Kihlberg, MD, MSPH, FACPM Department of Family and Community Medicine, Baylor College of Medicine, Houston, Tex (Dr. Zoorob); Department of Family and Community Medicine, Meharry Medical College, Nashville, Tenn (Drs. Chakrabarty, O’Hara, and Kihlberg) roger.zoorob@bcm.edu
The authors reported no potential conflict of interest relevant to this article. This article was made possible by grant number IM0HP25099 from the Health Resources and Services Administration (HRSA) Integrative Medicine Program. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of HRSA.
Exact dosages for probiotics have not been established, and recommendations range from 5 billion to 40 billion colony-forming units/d.22 The most commonly used probiotics are from the Lactobacillus and Saccharomyces genera; relatively little evidence supports other genera.21,22,35,36
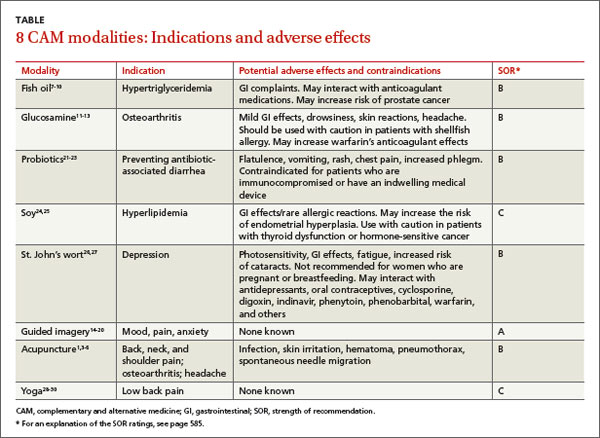
Probiotics are considered relatively safe, but are not recommended for patients who are immunocompromised or have an indwelling medical device.23 Adverse effects are rare, but may include flatulence, vomiting, rash, chest pain, and increased phlegm.21
Soybeans are a species of legume that contain significant amounts of protein, fiber, potassium, and iron. Although soy has been used to prevent or treat cancer, osteoporosis, and menopausal symptoms, current evidence is unfavorable or inconclusive for such conditions. Some RCTs have found soy has small, favorable effects on serum levels of low-density lipoprotein and total cholesterol,24 while others have shown modest improvements in triglyceride levels without significant improvements in other lipid levels.25
A 2011 meta-analysis of 10 RCTs that included 268 participants found that a diet high in non-soy legume products, such as alfalfa, lentils, and other beans, also improved lipid levels.37 A review of 136 studies that described 22 dietary interventions concluded that among other helpful dietary approaches to controlling hyperlipidemia, dietary soy—which contains fiber and polyunsaturated fats—is favored over supplementation of soy protein alone.38
Use caution when recommending soy for patients with thyroid dysfunction or hormone-sensitive cancers because some evidence suggests soy may interfere with absorption of levothyroxine and increase the risk of developing clinical symptoms of hypothyroidism.39
Soy also contains phytoestrogens, and prolonged use of soy supplements may increase the risk of endometrial hyperplasia.24 This risk has been documented only in the use of soy supplements, and not from dietary soy. GI disturbances and rare allergic reactions also have been reported.24
St. John’s wort for depression
Hypericum perforatum (St. John’s wort), a perennial herb, has been used to treat mood disorders and other ailments for more than 2000 years.40,41 Commercial preparations typically are alcohol extracts with an herb-to-extract ratio of 4:1 to 8:1.26 The normal dose ranges from 900 to 1500 mg/d in 2 to 3 divided doses of the alcohol extract standardized to 0.3% hypericin and/or 3% to 5% hyperforin.
St. John’s wort has been studied extensively as a treatment for depressive disorders. A 2001 double-blind RCT conducted in 11 US academic medical centers and community clinics between 1998 and 2000 that included 200 patients found that St. John’s wort was not effective for moderately severe major depression; a trend toward a positive effect was noted in both the placebo and St. John’s wort groups.26
However, a 2009 Cochrane review of 29 international studies (5489 patients) concluded that St. John’s wort may be better than placebo and as effective as antidepressants for mild to moderate major depression,27 and appeared to have fewer side effects than antidepressants. This review, conducted in German-speaking countries where medical professionals have long prescribed St. John’s wort, reported more positive results than those conducted in other countries.
St. John’s wort interacts with many medications, including antidepressants, oral contraceptives, cyclosporine, digoxin, indinavir, phenytoin, phenobarbital, warfarin, and others. It induces cytochrome P450 (CYP450) enzymes, and therefore can potentially reduce the efficacy of any medication that is metabolized by a CYP450 enzyme. When used in high doses in combination with antidepressants, St. John’s wort may cause serotonin syndrome. Other side effects include photosensitivity, GI complaints, fatigue, and increased risk of cataracts. Due to a lack of clinical data, St. John’s wort is contraindicated in women who are pregnant or breastfeeding.42
Motivational interviewing for substance abuse
Motivational interviewing (MI) is an alternative approach to traditional provider-patient communication that entails using open-ended questions, reflective listening, affirmation, and assessing readiness to change.1 MI facilitators aim to elicit change and assist patients in forming a self-management plan with specific, measurable, achievable, realistic, and timely (SMART) goals.1-3
MI can be efficiently implemented in diverse settings and by a variety of trained facilitators.3-5 For example, the Brief Negotiation Interview requires only 7 minutes per emergency department patient and effectively improves long-term outcomes for substance abusers.4 A randomized controlled trial that included 135 patients admitted to a psychiatric emergency inpatient unit for substance abuse found that those who received 2 sessions of MI reported significantly less substance use than controls 2 years after the intervention.3
Training for providers to ensure proper implementation of MI techniques is essential because poor use of MI can be counter-therapeutic.5 Tools such as the Motivational Interviewing Treatment Integrity Scale and the Client Evaluation of Motivational Interviewing can be used to ensure providers are competent.4,6
References
1. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behavior. New York, NY: Guilford Press; 1991.
2. Levensky ER, Forcehimes A, O’Donohue WT, et al. Motivational interviewing: an evidence-based approach to counseling helps patients follow treatment recommendations. Am J Nurse. 2007;107:50-59.
3. Bagøien G, Bjørngaard JH, Østensen C, et al. The effects of motivational interviewing on patients with comorbid substance use admitted to a psychiatric emergency unit - a randomized controlled trial with two year follow-up. BMC Psychiatry. 2013;13:93.
4. D’Onofrio G, Fiellin DA, Pantalon MV, et al. A brief intervention reduces hazardous and harmful drinking in emergency department patients. Ann Emerg Med. 2012;60:181-192.
5. Tollison SJ, Mastroleo NR, Mallett KA, et al. The relationship between baseline drinking status, peer motivational interviewing microskills, and drinking outcomes in a brief alcohol intervention for matriculating college students: a replication. Behav Ther. 2013;44:137-151.
6. Madson MB, Mohn RS, Zuckoff A, et al. Measuring client perceptions of motivational interviewing: factor analysis of the Client Evaluation of Motivational Interviewing scale. J Subst Abuse Treat. 2013;44:330-335.