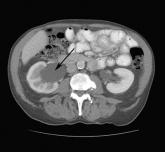
This patient was admitted to the hospital for further work-up and was subsequently told that he had duodenal perforation caused by indomethacin. Computed tomography scans revealed inflammation (arrows) and thickening of the second and third portion of the duodenum and the presence of extraluminal air at the perforation. Fluid was found along the right paracolic gutter and into the pelvis. The perforation was most likely caused by a nonsteroidal anti-inflammatory drug (NSAID)-induced ulcer.
Gastroduodenal damage is a well-known adverse effect of NSAIDs. NSAIDs inhibit cyclooxygenase (COX). The COX-1 enzyme is responsible for the production of prostaglandins, which play an important role in protecting the gastrointestinal (GI) mucosa. Ulcers in the GI tract can be complicated by perforation. Patients at risk for NSAID-related GI complications can benefit from the use of prophylactic agents, such as a proton pump inhibitor.
Suspect a possible perforation in the GI tract in patients who experience sudden onset of severe abdominal pain that may initially present as epigastric pain and progress to generalized abdominal pain that may radiate to one or both shoulders. Physical exam findings may include abdominal tenderness and a rigid abdomen, as well as fever and tachycardia.
A patient with a GI tract perforation must first be stabilized to determine if he or she requires surgical intervention (for patients whose perforation results in a persistent air leak) or medical management (for patients whose perforation is healing). In this case, the patient’s duodenal perforation was healing, so he was started on esomeprazole, ciprofloxacin, and metronidazole, and was scheduled for an outpatient endoscopy exam.
Adapted from: Singh M, Reichert P, Cann H. Photo Rounds: abrupt onset of abdominal pain. J Fam Pract. 2013;62:749-751.