John W. Epling, MD, MSEd Margot L. Savoy, MD, MPH Jonathan L. Temte, MD, PhD Bellinda K. Schoof, MHA, CPHQ Douglas Campos-Outcalt, MD, MPA State University of New York, Upstate Medical University, Syracuse (Dr. Epling); Christiana Care Health System, Wilmington, Del (Dr. Savoy); University of Wisconsin, Madison (Dr. Temte); American Academy of Family Physicians, Leawood, Kan (Ms. Schoof); Mercy Care Plan, Phoenix, Ariz (Dr. Campos-Outcalt) eplingj@upstate.edu
The authors produced this work as part of the American Academy of Family Physicians Vaccine Science Fellowship, which was funded by an unrestricted educational grant from Merck, Inc.
Persistent unfounded fear of vaccines and a belief that vaccine-preventable diseases are no longer a threat lead too many individuals to opt out.
› Reassure parents that vaccines are some of the safest and most effective interventions we have to prevent infectious disease. A › Advise parents that there are multiple systems in place to monitor vaccine safety. C › Educate parents that lapses in immunization rates can put children at risk of resurgent cases of previously well-controlled diseases, like measles and Haemophilus influenza type b. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence B Inconsistent or limited-quality patient-oriented evidence C Consensus, usual practice, opinion, disease-oriented evidence, case series
When a public health intervention succeeds and achieves long-term suppression of the target problem, an unfortunate irony is that, with time, the intervention can seem less vital. So it is with vaccines. Many patients and physicians today have never experienced the infectious diseases that once caused millions of deaths and much disability each year, and they therefore do not appreciate the impact these diseases had when they were prevalent.
It is estimated that just 9 of the routinely recommended vaccines prevent 42,000 deaths and 20 million cases of disease in every birth cohort.1 With many of these diseases thus held at bay, attention shifted instead to the supposed risks of vaccines. Many people mistakenly believe a vaccine’s potential for harm is more likely than the chance of acquiring the disease it prevents, and they therefore refuse vaccines for themselves and their children, with little chance in the short term of suffering an adverse outcome for their decision.
In this review—which can inform primary care physicians’ discussions with vaccine-hesitant patients—we first highlight 2 preventable diseases, measles and Haemophilus influenzae type b (Hib) infection. Recent residency graduates may never see these diseases thanks to sustained vaccination programs. However, the risk of acquiring these infections has not disappeared entirely. After considering these examples, we examine the totality of the morbidity and mortality prevented by vaccination and describe the safety of current vaccines and the systems in place to assure their continued safety.
Measles: No longer endemic to the United States, but still a risk from importation
In the pre-vaccine era, measles (rubeola) infected more than 500,000 Americans annually and killed roughly 500.2 This highly communicable systemic acute viral infection was once considered universal in childhood. After vaccine licensure in 1963, widespread immunization reduced the incidence by more than 98%, and by 2000 it had eliminated endemic measles from the United States. However, the disease has now reappeared—largely due to international travel and neglect in becoming vaccinated. As of October 31, 2014, the United States had 20 outbreaks and 603 cases of measles reported in 2014—a dramatic increase over recent years.3
Clinical appearance. Acute measles infection is characterized by high fever, cough, coryza, conjunctivitis, and rash. Koplik spots are a 24- to 72-hour pathognomonic exanthem of blue-white spots 1 to 3 mm in diameter on an erythematous base along the buccal mucosa. The resolving exanthem coincides with the eruption of a blanching, maculopapular exanthem originating at the hairline, progressing down the trunk and out to the limbs (sparing the palms and soles), coalescing, and then fading with a fine desquamation in the same order of appearance over 7 days. Additional associated symptoms include anorexia, diarrhea, and generalized lymphadenopathy.2,4
Complications are common with measles. Acute measles infection is rarely fatal. However, serious complications occur in nearly one-third of reported cases.2 During the 1989-1991 measles resurgence in the United States, more than 100 deaths occurred among the 55,000 cases reported.5-7 In early 2011, the United States saw the highest reported number of measles cases since 1996 due to importation. Of the 118 reported cases, 105 (89%) occurred in unvaccinated people, 47 (40%) required hospitalization, and 9 individuals developed pneumonia.8
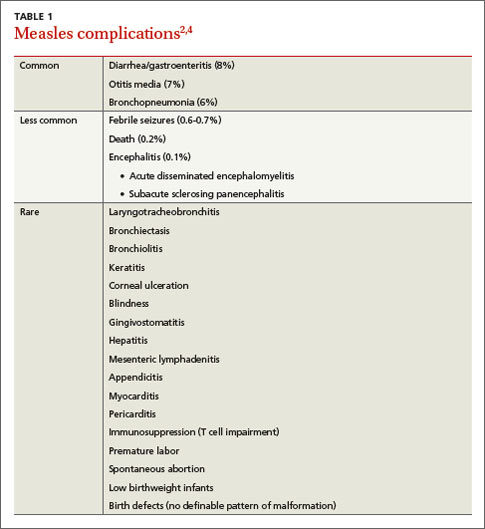
While acute measles is rarely fatal, serious complications occur in nearly one-third of cases. Complications of measles infection are shown in TABLE 1.2,4 Pneumonia (viral or superimposed bacterial) accounts for 60% of measles-related deaths.2 Neurologic complications, while less frequent, can be severe.
Acute encephalitis occurs in 1 in 1000 to 2000 cases and presents within a week following the exanthem with fever, headache, vomiting, meningismus, change in mental status, convulsions, and coma.2 Encephalitis has a fatality rate of 15%, leaving another 25% with residual neurologic damage.2 Subacute sclerosing panencephalitis (SSPE) occurs in 5 to 10 cases per million (in the United States), on average 7 years after the initial measles infection.9,10 After an insidious onset, behavior and intellect deteriorate, followed by ataxia, myoclonic seizures, and ultimately death. In the United States, the number of reported cases of SSPE has declined with the reduction in measles cases. However, in countries with less robust measles immunization eradication programs, the risk of developing SSPE remains.9,10