Linda Speer, MD Saudia Mushkbar, MD Department of Family Medicine, University of Toledo College of Medicine and Life Sciences, Ohio (Drs. Speer and Mushkbar) linda.speer@utoledo.edu
The authors reported no potential conflict of interest relevant to this article.
Recent advances in our understanding of the pathophysiology of chronic fatigue and related disorders can help guide your response to this common complaint.
CASE › Lauren C, age 35, comes to the clinic because of fatigue, which she says started at least 8 months ago and has gotten progressively worse. The patient, a clerical worker, says she manages to do an adequate job but goes home feeling utterly exhausted each night.
Ms. C says she sleeps well, getting more than 8 hours of sleep per night on weekends but fewer than 7 hours per night during the week. But no matter how long she sleeps, she never awakens feeling refreshed. Ms. C reports that she doesn’t smoke, has no more than 4 alcoholic drinks per month, and adheres to an “average” diet. She is too tired to exercise.
Ms. C is single, with no children. Although she says she has a strong network of family and friends, she increasingly finds she has no energy for socializing. If Ms. C were your patient, what would you do?
Patients with an organ-based medical illness tend to associate their fatigue with activities that they are unable to complete, while those with fatigue that is not organ-based typically say that they're tired all the time.Fatigue is a common presenting symptom in primary care, accounting for about 5% of adult visits.1 Defined as a generalized lack of energy, fatigue that persists despite adequate rest or is severe enough to disrupt an individual’s ability to participate in key social and/or occupational activities warrants a thorough investigation.
Because fatigue is a nonspecific symptom that may be linked to a number of medical and psychiatric illnesses or medications used to treat them, determining the cause can be difficult. In about half of all cases, no specific etiology is found.2 This review, which includes the elements of a work-up and management strategies for patients presenting with ongoing fatigue, will help you arrive at the appropriate diagnosis and provide optimal treatment.
Chronic fatigue: Defining the terms
A definition of chronic fatigue syndrome (CFS) was initially published in 1988.3 In subsequent years, the term myalgic encephalomyelitis (ME) became popular. Although the terms are sometimes used interchangeably, ME often refers to patients whose condition is thought to have an infectious cause and for whom postexertional malaise is a hallmark symptom.4
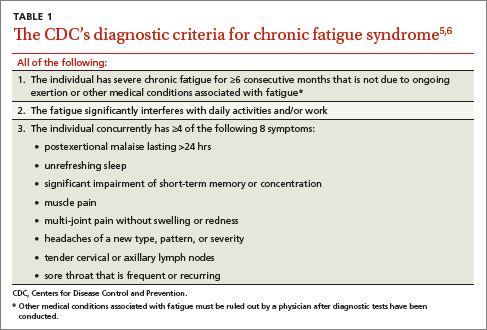
CDC criteria. While several sets of diagnostic criteria for CFS have been developed, the most widely used is that of the Centers for Disease Control and Prevention (CDC), published in 1994 (TABLE 1).5,6 A diagnosis of CFS is made on the basis of exclusion, subjective clinical interpretation, and patient self-report.
When the first 2 criteria—fatigue not due to ongoing exertion or other medical conditions that has lasted ≥6 months and is severe enough to interfere with daily activities—but fewer than 4 of the CDC’s 8 concurrent symptoms (eg, headache, unrefreshing sleep, and postexertion malaise lasting >24 hours) are present, idiopathic fatigue, rather than CFS, is diagnosed.6
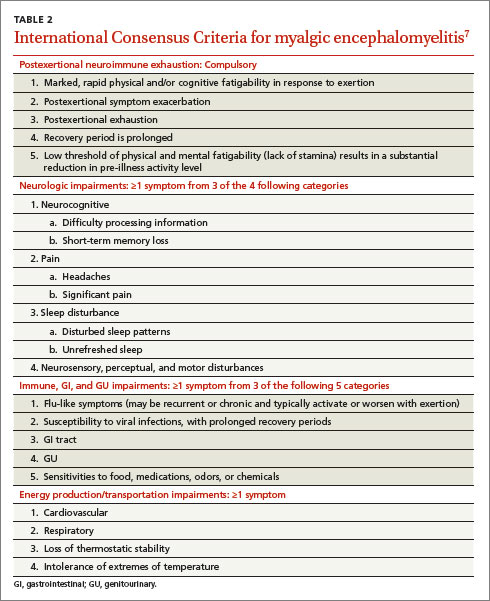
International Consensus Criteria (ICC). In 2011, the ICC for ME were proposed in an effort to provide more specific diagnostic criteria (TABLE 2).7 The ICC emphasize fatigability, or what the authors identify as “post-exertional neuroimmune exhaustion.”
The ICC have not yet been broadly researched. But an Australian study of patients with chronic fatigue found that those who met the ICC definition were sicker and more homogeneous, with significantly lower scores for physical and social functioning and bodily pain compared with those who fulfilled the CDC criteria alone.8
Chronic fatigue & neuropsychiatric conditions: Common threads
Recent research has made it clear that depression, somatization, and CFS share some biological underpinnings. These include biomarkers for inflammation, cell-mediated immune activation—which may be related to the symptoms of fatigue—autonomic dysfunction, and hyperalgesia.9 Evidence suggests that up to two-thirds of patients with CFS also meet the criteria for a psychiatric disorder.10 The most common psychiatric conditions are major depressive disorder (MDD), affecting an estimated 22% to 32% of those with CFS; anxiety disorder, affecting about 20%; and somatization disorder, affecting about 10%—at least double the incidence of the general population.10
Others point out, however, that up to half of those with CFS do not have a psychiatric disorder.11 A diagnosis of somatization disorder, in particular, depends largely on a subjective interpretation of whether or not the presenting symptoms have a physical cause.10
CFS and MDD comorbidity. The most widely studied association between CFS and psychiatric disorders involves MDD. Observational studies have found patients with CFS have a lifetime prevalence of MDD of 65%,12,13 which is higher than that of patients with other chronic diseases. Overlapping symptoms include fatigue, sleep disturbance, poor concentration, and memory problems. However, those with CFS have fewer symptoms related to anhedonia, poor self-esteem, guilt, and suicidal ideation compared with individuals with MDD.12,13