Dr. Moon is a Fellow in the Division of Gastroenterology and Hepatology at University of North Carolina School of Medicine in Chapel Hill, North Carolina. Dr. Lowy is a Data Analyst for the HHRC Data and Analytics Group and Data Analyst for Health Services Research and Development at VA Puget Sound Healthcare System. Dr. Chartier is the Deputy Director and the National Infectious Diseases Officer for the Veterans Health Administration (VHA), Office of Specialty Care Services, HIV, Hepatitis, and Related Conditions Programs (HHRC). Dr. Beste is a Staff Physician and the Director of the VA National Liver Disease Database at VA Puget Sound Healthcare System, the Director of the HHRC Data Analytics Group, and Assistant Professor of Medicine in the Division of General Internal Medicine at the University of Washington in Seattle. Dr. Maier is a Staff Physician in the Infectious Diseases Section at VA Portland Healthcare System in Oregon and an Assistant Professor in the Division of Infectious Diseases at Oregon Health and Sciences University in Portland. Dr. Maier is the National Public Health Infectious Disease Officer. Dr. Morgan is the Director of the HHRC National Hepatitis Resource Center; Chief, Gastroenterology at VA Long Beach Healthcare System in California; and Professor in the Division of Gastroenterology at University of California, Irvine. Ms. Hoffman-Högg is National Program Manager for Prevention Policy at VHA National Center for Health Promotion and Disease Prevention in Durham, North Carolina Correspondence: Dr. Moon (andrew.moon@unchealth.unc.edu)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
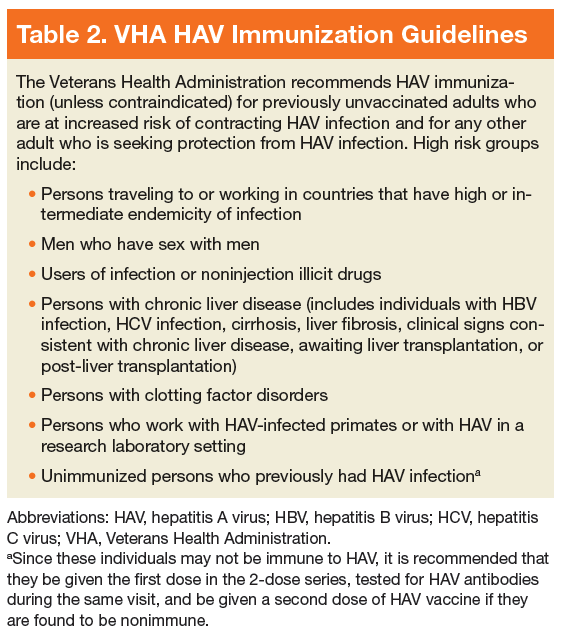
The mainstay of HAV prevention is vaccination with 2 doses of inactivated, single-antigen hepatitis A vaccine or 3 doses of combination (HAV and HBV) vaccine.11 Both single antigen and combination HAV vaccines are safe in immunocompromised and pregnant patients.33-39 The HAV vaccination results in 100% anti-HAV IgG seropositivity among healthy individuals, although immunogenicity might be lower for those who are immunocompromised or with CLD.31,40-47 The VHA recommends HAV immunization, unless contraindicated, for previously unvaccinated
adults who are at increased risk of contracting HAV and for any other adult who is seeking protection from HAV infection (Table 2).48 Hepatitis A virus vaccination is not specifically recommended for workers in food service, health care, sanitation, or child care.11
In addition to vaccination, addressing risk factors for HAV infection and its complications could reduce the burden of disease. For instance, recent outbreaks highlight that homeless individuals and users of injection and noninjection drugs are particularly vulnerable to infections transmitted via fecal-oral contamination. Broad strategies to address homelessness and related sanitation concerns are needed to help reduce the likelihood of future HAV outbreaks.49 Specific measures to combat HAV include providing access to clean water, adequate hygiene, and clean needles for people who inject drugs.11 Hepatitis A virus can be destroyed by heating food to ≥ 185 °F for at least 1 minute, chlorinating contaminated water, or cleaning contaminated surfaces with a solution of household bleach and water.50 Moreover, it is important to identify and treat risk factors for complications of HAV infection. This includes identifying individuals with HCV and ensuring that they are immune to HAV, given data that HCV-infected individuals are at increased risk of fulminant hepatic failure from HAV.12,13
Active-duty service members have long been considered at higher risk of HAV infections due to deployments in endemic areas and exposure to contaminated food and water.51,52 Shortly after the FDA approved HAV vaccination in 1995, the Department of Defense (DoD) mandated screening and HAV immunization for all incoming active-duty service members and those deployed to areas of high endemicity.53 However, US veterans who were discharged before the adoption of universal HAV vaccination remain at increased risk for HAV infection, particularly given the high prevalence of CLD, homelessness, and substance use disorder (SUD) in this cohort.54-56 Given the importance of HAV prevention for high-risk individuals, an analysis was performed to determine rates of HAV vaccination and testing within VA-enrolled individuals with selected risk factors for HAV acquisition or complications.
Methods
A cross-sectional analysis of veterans in VA care from June 1, 2016 to June 1, 2017 was performed to determine national rates of HAV susceptibility among patients with HCV exposure, homelessness, SUD, or HIV infection. The definitions of homelessness, SUD (alcohol, cannabis, opioid, sedatives, hallucinogens, inhalants, stimulants, or tobacco), and HIV infection were based on the presence of appropriate ICD-9 or ICD-10 codes. History of HCV exposure was based on a positive HCV antibody test. Presence of HAV vaccination was determined based on CPT codes for administration of the single-antigen HAV vaccination or combination HAV/HBV vaccination.
While HIV infection is not independently considered an indication for HAV vaccination, the authors included this group given its high proportion of patients with other risk factors, including MSM and IV drug use. All data were obtained from the VA Corporate Data Warehouse (CDW), a comprehensive national repository of all laboratory, diagnosis, and prescription results (including vaccines) within the VHA since 1999.
Hepatitis A virus nonsusceptibility was defined as (1) documented receipt of HAV vaccination within the VHA; (2) anti-HAV IgG antibody testing within the VHA; or (3) active-duty service after October 1997. It was considered likely that patients who received HAV testing either showed evidence of HAV immunity (eg, positive anti-HAV IgG) or were anti-HAV IgG negative and subsequently immunized. Therefore, patients with anti-HAV IgG antibody testing were counted presumptively as nonsusceptible. The DoD implemented a universal HAV vaccination policy in 1995, therefore, 1997 was chosen as a time at which the military’s universal HAV vaccination campaign was likely to have achieved near 100% vaccination coverage of active-duty military.
Results
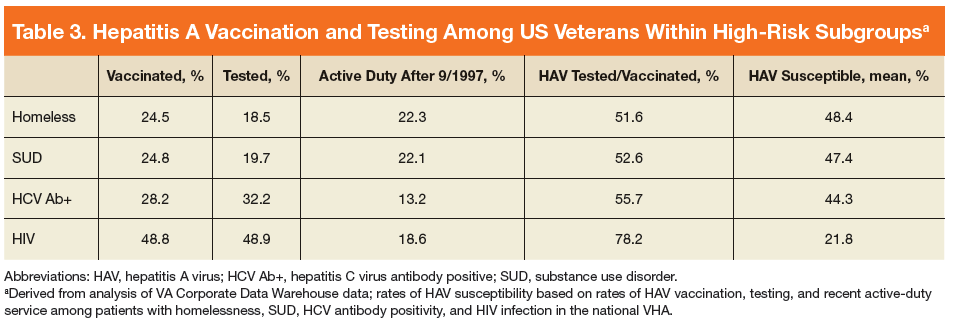
The cohort included 5,896,451 patients in VA care, including 381,628 (6.5%) who were homeless, 455,344 (7.7%) with SUD, 225,889 (3.8%) with a lifetime history of positive HCV antibody (indicating past HCV exposure), and 29,166 (0.5%) with HIV infection.
National rates of HAV susceptibility were lowest among patients with HIV (mean 21.8%, facility range 0%-56.5%) followed by SUD (mean 47.4%, facility range 3.8%-70.4%), homelessness (mean 48.4%, facility range 5.9%-69.3%), and HCV exposure (mean 48.9%, facility range 30.5%-71.6%) (Table 3).