Dr. Moon is a Fellow in the Division of Gastroenterology and Hepatology at University of North Carolina School of Medicine in Chapel Hill, North Carolina. Dr. Lowy is a Data Analyst for the HHRC Data and Analytics Group and Data Analyst for Health Services Research and Development at VA Puget Sound Healthcare System. Dr. Chartier is the Deputy Director and the National Infectious Diseases Officer for the Veterans Health Administration (VHA), Office of Specialty Care Services, HIV, Hepatitis, and Related Conditions Programs (HHRC). Dr. Beste is a Staff Physician and the Director of the VA National Liver Disease Database at VA Puget Sound Healthcare System, the Director of the HHRC Data Analytics Group, and Assistant Professor of Medicine in the Division of General Internal Medicine at the University of Washington in Seattle. Dr. Maier is a Staff Physician in the Infectious Diseases Section at VA Portland Healthcare System in Oregon and an Assistant Professor in the Division of Infectious Diseases at Oregon Health and Sciences University in Portland. Dr. Maier is the National Public Health Infectious Disease Officer. Dr. Morgan is the Director of the HHRC National Hepatitis Resource Center; Chief, Gastroenterology at VA Long Beach Healthcare System in California; and Professor in the Division of Gastroenterology at University of California, Irvine. Ms. Hoffman-Högg is National Program Manager for Prevention Policy at VHA National Center for Health Promotion and Disease Prevention in Durham, North Carolina Correspondence: Dr. Moon (andrew.moon@unchealth.unc.edu)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
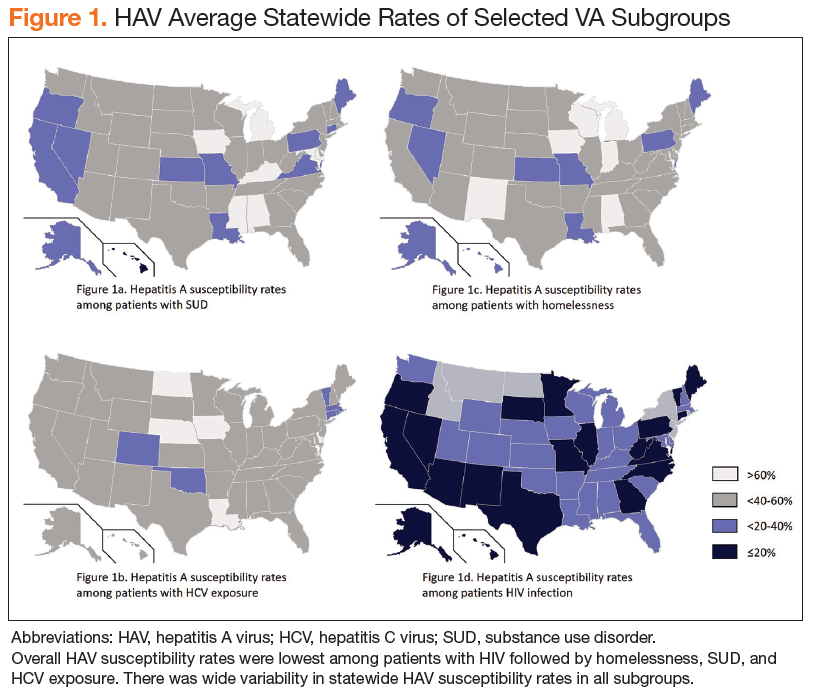
There was wide geographic variability in rates of HAV susceptibility (Figure 1).
When limiting the analysis to patients with confirmed vaccination within the VHA or active duty military service after October 1997, VA facilities in states with active outbreaks had a mean HAV vaccination rate of 38.1% (range 31.5%-44.3%) among patients who were homeless and 42.0% (range 33.8%-49.0%) among patients with SUD.
Discussion
Widespread HAV vaccination has decreased the incidence of HAV infection in the US dramatically. Nevertheless, recent outbreaks demonstrate that substantial population susceptibility and associated risk for HAV-related morbidity and mortality remains, particularly in high-risk populations. Although the VHA has not experienced a significant increase in acute HAV infections to date, this cross-sectional analysis highlights that a large proportion of VA patients in traditionally high-risk groups remain susceptible to HAV infection.
Strengths
Strengths of this analysis include a current reflection of HAV susceptibility within the national VHA, thus informing HAV testing and vaccination strategies. This study also involves a very large cohort, which is possible because the VHA is the largest integrated healthcare system in the US. Lastly, because the VHA uses electronic medical records, there was nearly complete capture of HAV vaccinations and testing obtained through the VHA.
Limitations
This cross-sectional analysis has several potential limitations. First, findings may not be generalizable outside the VHA. In addition, determination of homelessness, substance abuse, and HIV infection were based on ICD-9 and ICD-10 codes, which have been used in previous studies but may be subject to misclassification. The authors deliberately included all patients with positive HCV antibody testing to include those with current or prior risk factors for HAV acquisition. This population does not reflect patients with HCV viremia who received HAV testing or vaccination. Lastly, misattribution of HAV susceptibility could have occurred if patients with negative HAV IgG results were not vaccinated or if patients previously received HAV vaccination outside the VHA.
Conclusion
To mitigate the risk of future HAV outbreaks, continued efforts should be made to increase vaccination among high-risk groups, improve awareness of additional prevention measures, and address risk factors for HAV acquisition, particularly in areas with active outbreaks. Further study is suggested to identify geographic areas with large caseloads of at-risk patients and to highlight best practices utilized by VHA facilities that achieved high vaccine coverage rates. Recommended approaches likely will need to include efforts to improve hygiene and reduce risks for HAV exposure associated with SUD and homelessness.