References
- DiVenere L. The Affordable Care Act: What’s the latest? OBG Manag. 2014;26(10):36–42.
- Guttmacher Institute. A real-time look at the impact of the recession on women’s family planning and pregnancy decisions, 2009. http://www.guttmacher.org/pubs/RecessionFP.pdf. Published September 2009. Accessed October 6, 2014.
- Liang SY, Grossman D, Phillips KA. Women’s out-of-pocket expenditures and dispensing patterns for oral contraceptive pills between 1996 and 2006. Contraception. 2011;83(6):528–536.
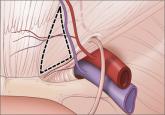
While I found the article “Update on operative vaginal delivery” by Dr. Errol Norwitz very informative, I would like to inject what I hope is a little common sense into the warning to only attempt operative delivery with either forceps or vacuum, never both.
My objection to this rule is that it ignores those situations where the vacuum is used for a vertex slightly above the perineum, when the head descends easily to the introitus, but, because of caput and molding, cannot be delivered because adequate vacuum cannot be maintained. I believe an outlet forceps delivery in this situation is more justified than a trip to the OR for cesarean delivery. An outlet forceps delivery can resolve the concern about the infant’s health faster than would a cesarean delivery.
E. Darryl Barnes, MD
Richmond, Virginia
I’d like to thank Dr. Barnes for his interest and his comments. The decision to perform a forceps delivery after a failed vacuum extraction should be taken with extreme caution. The literature is clear that such deliveries are associated with a high risk of birth injury. While it is true that, in select cases, such an approach may expedite delivery sooner than an emergency cesarean and, as such, could be seen as a reasonable option under the circumstances, this decision may prove difficult to defend should a birth injury result. Might I suggest that providers reach first for the forceps.
Share your thoughts on these letters or another article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.