The cycle of addiction
The validity of a medical diagnosis is based on patterns of family history, prognosis, treatment response, and course of disease. Sexual addiction, with its predictable course and family history, may meet these diagnostic criteria.
Sexual addicts, like mythical vampires, lead secret lives designed to feed the addiction process rather than life itself. The planning, arrangements, cruising, and cover-ups compete for time with family, friends, career, and hobbies. This creates a chronic situation of unmanageability of circumstances. To cope, the addict creates a strange belief system, such as the pedophile priest’s belief that sex between men and boys is natural and that the trauma lies in reporting and investigating it.9 Belief systems such as these are often socially supported by organizations and in publications by like-minded persons.
Self-interested distortions lead the addict to wrongly perceive that victims are cooperating and the self and others are not being harmed. The result is often gross misinterpretations of reality, such as the man who thinks he is flirting at the office but is charged with sexual exploitation by a co-worker. A sequence of mental events (Figure 1) leads to, and helps the addict cope with, the addiction cycle.
The addiction cycle Carnes describes a four-stage addiction cycle: preoccupation, ritualization, sexual acting out, and despair (Figure 2). Stressful or painful experiences—a narcissistic injury, a disappointment, stress-related anxiety—or the boredom and emptiness of unstructured time may initiate the sequence. The sufferer learns, through repetitive trials and reinforcement mechanisms, to take the maladaptive path into the addiction cycle rather than making a healthy emotional adaptation.
Reasons why one person takes the path to addiction when others do not may include genetics (emotional temperament), developmental and familial circumstances, and state-dependent learning. However the cycle is entered, the preoccupation stage begins the action that characterizes all addictions—diversion of attention from the painful state and anticipation of relief or pleasure.
With all addictive substances, the preoccupation phase exhibits tolerance. Longer time frames require higher doses, and increased stimulation of ritualization is required to produce the same mood-altering effect. The addict begins to devote increasing time and energy to the addiction, consuming resources that persons around him or her realize would be better invested in friends, family, career, or recreation (real life).
It is overstatement to characterize the patient’s denial and distortions as thought disorder. Nevertheless, many patients report waking as if from a dream to realize how their perceptions, rationalizations, and behavior have become inconsistent with their own long-held values and sense of reality.
The acting-out phase is often followed by a brief sense of relief and return to normal thinking which—paradoxically—obscure the emergence of despair and rekindling of the addictive cycle. The psychological phase of despair has several important clinical implications. In alcohol addiction, for example, pseudodepression in a freshly detoxified alcoholic often resolves with abstinence. When superimposed on clinical depression, the phase may take on vegetative signs and symptoms, with dangerously increased suicide potential.
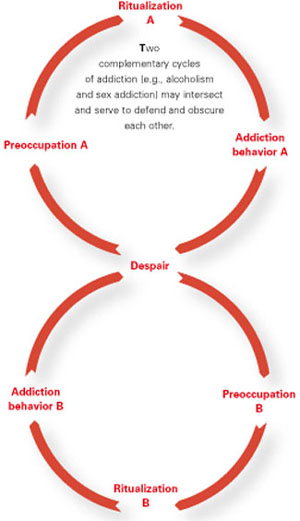
Multiple addictions Another fascinating possibility is the generic nature of the despair phase as opposed to the preoccupation phase. It opens the door to mixed or multiple addictions, in which several addiction cycles are linked and serve to defend and obscure each other (Figure 3).
An example is the alcoholic sex addict who is promiscuous after an alcohol binge. He may explain his drinking at a party as a reaction to the presence of several previous sex partners and attribute his promiscuity to intoxication. Thus, the addiction process underlying both behaviors is concealed, as is the functional relationship between the two. Often there is partial awareness (e.g., the alcohol/sex addict has noticed that his promiscuous acting out frequently occurs after, but only rarely during, an intoxication episode).
Figure 1 BELIEF AND THINKING CYCLE OF SEXUAL ADDICTION
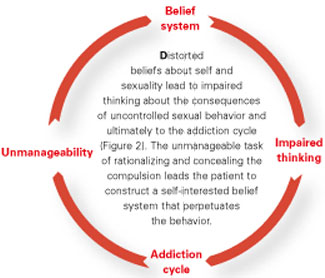
Figure 2 FOUR-STAGE SEXUAL ADDICTION CYCLE

Figure 3 MULTIPLE-ADDICTION CYCLE
Recognizing symptoms
The diagnosis of sexual addiction is often made by the patient who recognizes himself in a description of the cycle of addictive thoughts and behavior. Many patients report being aware that their thinking is distorted or their behavior is out of control. They often can admit that their behavior is inconsistent with their values.
Screening For clinicians, what are the diagnostic signs of sexual addiction? Numbers of sex partners or frequency of sex may not provide adequate information or reliable criteria. The 25 items on Carnes’ Sexual Addiction Screening Test (SAST)6 bring previously off-the-radar subjects into consideration. For example, questions on the survey include:
- Have you subscribed to or regularly purchased sexually explicit magazines like Playboy or Penthouse?
- Do you ever feel bad about your sexual behavior?
- Have you made promises to yourself to quit some aspect of your sexual behavior?6