PRACTICE RECOMMENDATIONS
› Use provocative testing to confirm a suspected diagnosis in a patient who presents with peripheral entrapment mononeuropathy. B
› Consider electrodiagnostic testing for help in diagnosing a challenging presentation, ruling out a competing diagnosis, or clarifying an atypical clinical picture or vague subjective history. A
› Evaluate any patient who presents with non-anatomic nerve distribution of symptoms—eg, burning, numbness, and tingling of the entire hand—for a metabolic, rather than an entrapment, neuropathy. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Neuropathic hand complaints—for which patients typically seek medical attention when the pain or paresthesia starts to interfere with their daily routine—are common and diverse. The ability to assess and accurately diagnose upper extremity compression neuropathies is critical for physicians in primary care.
Assessment starts, of course, with a thorough history of the present illness and past medical history, which helps define a broad differential diagnosis and identify comorbidities. Physical examination, including judicious use of provocative testing, allows you to objectively identify the pathologic deficit, evaluate function and coordination of multiple organ systems, and detect nerve dysfunction. The results determine whether additional tools, such as electrodiagnostic testing, are needed.
We’ve created this guide, detailed in the text, tables, and figures that follow, to help you hone your ability to accurately diagnose patients who present with compression neuropathies of the hand.
The medical history: Knowing what to ask
To clearly define a patient’s symptoms and disability, start with a thorough history of the presenting complaint.
Inquire about symptom onset and chronicity. Did the pain or paresthesia begin after an injury? Are the symptoms associated with repetitive use of the extremity? Do they occur at night?
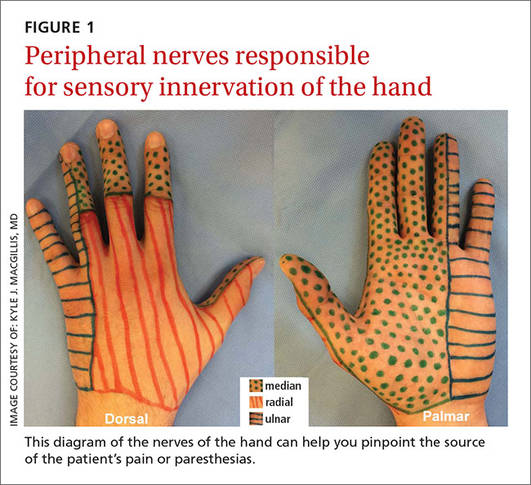
Pinpoint the location or distribution of pain or paresthesia. It is paramount to identify the affected nerve.1,2 Ask patients to complete a hand or upper extremity profile documenting location and/or type of numbness, tingling, or decreased sensation. A diagram of the peripheral nerves responsible for sensory innervation of the hand (FIGURE 1) is an effective way to screen individuals at high risk of carpal tunnel syndrome (CTS) or ulnar tunnel syndrome (UTS).1,2
A patient report such as, “My whole hand is numb,” calls for a follow-up question to determine whether the little finger is affected,3 which would indicate that the ulnar nerve, rather than just the median nerve, is involved. And if a patient reports feeling as if he or she is wearing gloves or mittens, it is essential to consider the possibility of a systemic neuropathy rather than a single peripheral neuropathy.3
Gather basic patient information. Inquire about hand dominance, occupation, and baseline function, any or all of which may be critical in the assessment and initiation of treatment.4,5
Review systemic conditions and medications

A broad range of comorbidities, such as cervical radiculopathy, diabetes, hypothyroidism, and vitamin deficiencies (TABLE 1),6,7 may be responsible for neuropathic hand complaints, and a thorough review of systemic complaints and past medical history is critical. Include a medication history and a review of prior procedures, such as post-traumatic surgeries of the hand or upper extremity or nerve decompression surgeries, which may provide additional insight into disease etiology.
Symptoms guide physical exam, provocative testing
A physical examination, including provocative testing, follows based on reported symptoms, medical history, and suspected source of nerve compression.
Carpal tunnel syndrome
CTS is the most common peripheral neuropathy.8 Patients often report nocturnal pain or paresthesia in the distal median nerve distribution, comprising the palmar surface of the thumb, index, middle, and radial half of the ring finger.
Researchers have identified 6 standardized clinical criteria for the diagnosis of CTS. Two criteria—numbness mostly in median nerve territory and nocturnal numbness—can be ascertained during the history of present illness.The other 4, detailed below, will be found during the physical exam.9
Thenar weakness or atrophy.9 Begin your evaluation by inspecting the thenar musculature for atrophic changes. Motor exam of intrinsic musculature innervated by the recurrent motor branch of the median nerve includes assessment of thumb abduction strength (assessed by applying resistance to the metacarpophalangeal joint [MCPJ] base towards the palm in the position of maximal abduction) and opposition strength (assessed by applying force to the MCPJ from the ulnar aspect).10
Positive Phalen’s test.9 Provocative testing for CTS includes Phalen’s test (sensitivity 43%-86%, specificity 48%-67%),11 which is an attempt to reproduce the numbness or tingling in the median nerve territory within 60 seconds of full wrist flexion. Ask the patient to hold his or her forearms vertically with elbows resting on the table (allowing gravity to flex the wrists),12 and to tell you if numbness or tingling occurs.
Positive Tinel’s sign.9 Tinel’s sign (sensitivity 45%-75%, specificity 48%-67%)11 is performed by lightly tapping the median nerve from the proximal to distal end over the carpal tunnel. The test is positive if paresthesia results. Provocative testing may also include Durkan’s test, also known as the carpal compression test. Durkan’s test (sensitivity 49%-89%, specificity 54%-96%)11 involves placing your thumb directly over the carpal tunnel and holding light compression for 60 seconds, or until paresthesia is reported.
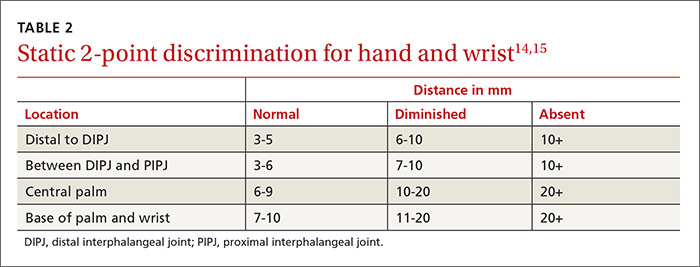
Positive 2-point discrimination test.9 To assess CTS disease severity, use 2-point discrimination to evaluate the patient’s sensation qualitatively and quantitatively. Two-point discrimination can only be tested, however, if light touch sensation is intact. It is typically performed by lightly applying 2 caliper points at fixed distances sufficient to blanch the skin, but some clinicians have used other tools, such as a modified paperclip.13 The smallest distance at which the patient can detect 2 distinct stimuli is then recorded.
Researchers have reported an average of 3 to 5 mm for 2-point discrimination at the fingertipand a normal 2-point discrimination of 6 to 9 mm in the volar surface of the hand (TABLE 2).14,15
The scratch collapse test (sensitivity 64%, specificity 99%) is a supplemental exam that uses a different outcome measure to diagnose CTS.16 It involves lightly scratching the skin over the compressed carpal tunnel while the patient performs sustained resisted bilateral shoulder external rotation in an adducted position. A momentary loss of muscle resistance to external rotation indicates a positive test.