
From the Journals
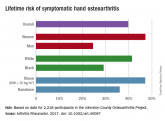
Lifetime risk of hand OA comes close to 40%
Risk approaches 50% for women and the obese, according to data from the Johnston County Osteoarthritis Project.
EULAR has updated its 2007 guidelines for the management of hand osteoarthritis. I find the recommendations helpful, and I have no disagreements.
The authors performed a systematic literature review that was more complete than the original guidelines. In addition, the methodology in developing the guidelines was updated utilizing the GRADE (Grading of Recommendations, Assessment, Development and Evaluations) system to guide the expert opinion. The manuscript presents recommendations that are carefully supported in the text. To understand guidelines, one really needs to read the text.

Dr. Roy D. Altman
The update lists a set of research questions, similar to the 2007 recommendations.
The authors group their therapeutic recommendations according to nonpharmacologic, pharmacologic, and surgical approaches, as well as about the need for follow-up. The three nonpharmacologic recommendations include education and training, exercise and muscle strengthening, and the use of orthoses. The pharmacologic approach includes topical therapy as a first-line, oral NSAIDs and analgesics, chondroitin sulfate, and intra-articular injections. There is a negative recommendation for the use of biologics. The surgical recommendation is directed at the relief of pain. The last recommendation emphasizes the need for follow-up and individual care.
The differences between the recommendations include the removal of acetaminophen as a first-line therapy. Indeed, it seems to be barely recommended at all. In addition, there is an emphasis on topical therapy, particularly NSAIDs. The authors are equivocal on the recommendations for intra-articular therapy. Paraffin and local heat are no longer included. The recommendation against biologic therapy is new. They included agents used for rheumatoid arthritis, such as methotrexate, in this negative recommendation.
These new recommendations are an update of guidelines that are over 10 years old. They are practical and helpful. Unfortunately, more research is needed as the present day therapy is often inadequate.
Roy D. Altman, MD, is professor emeritus of medicine in the division of rheumatology and immunology at the University of California, Los Angeles. He is a consultant to Ferring, Flexion, GlaxoSmithKline, Novartis, Olatec, Pfizer, and Sorrento Therapeutics.
FROM ANNALS OF THE RHEUMATIC DISEASES
Risk approaches 50% for women and the obese, according to data from the Johnston County Osteoarthritis Project.