A meta-analysis of 8 published studies involving 840 patients whose condition was not improved after conservative therapy for at least 6 months showed that up to 88% of patients experienced good to excellent outcomes with extracorporeal shock wave therapy and were satisfied with the result. 6
As for surgical treatment, in a prospective study of 43 patients with 47 painful heels followed for an average of 31 months, only 49% of the patients were satisfied with their outcome.8 Patient expectations should be considered in preoperative counseling. In contrast to surgery, either open or endoscopic, extracorporeal shock wave therapy does not require the patient avoid weightbearing or a prolonged time for return to work.
FIGURE 1
Tension night splinting
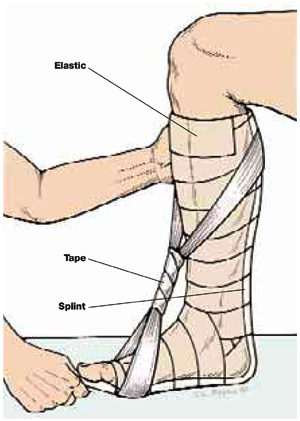
With the knee flexed 90°, secure the splint to the leg with elastic. Remove the splint and moisten, then reapply with the ankle at maximum dorsiflexion. Apply tape in a figure-8 until the fiberglass hardens.
Recommendations from others
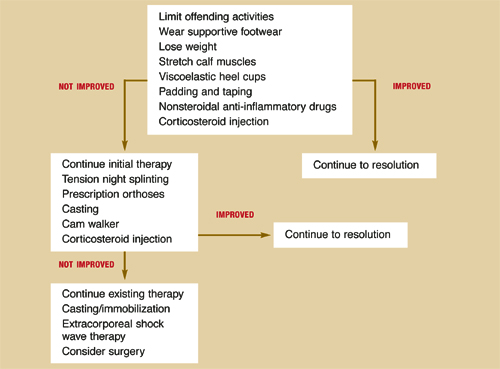
Figure 2 has been modified from a clinical practice guideline on the treatment of plantar fasciitis published by the American College of Foot and Ankle Surgeons.9
FIGURE 2
Treatment of plantar fasciitis
CLINICAL COMMENTARY
Keys to treatment: Avoid overuse, stabilize, be patient
Mark B. Stephens, MD, MS
Uniformed Services University of the Health Sciences, Bethesda, Md
Plantar fasciitis (heel pain syndrome) is one of the most common disorders of the foot and ankle and is notoriously difficult to treat. Patients are commonly symptomatic for months, leading to frustration, poor compliance, and general dissatisfaction.
From a pathophysiologic perspective, plantar fasciitis is a form of overuse syndrome. When approached in this manner, it makes intuitive (and now scientific) sense that stabilization of the proximal fascial enthesis at the point of its insertion to the calcaneus is the key to clinical resolution of symptoms. Activity modification, mechanical therapy, and patience are the essential elements for treating plantar fasciitis.