Interventions
Once the samples had been collected, patients were randomly assigned to oral treatment with either 500 mg amoxicillin 3 times daily for 10 days or 300 mg roxithromycin once daily for 10 days. A computer program using random permuted blocks of 6 prepared a randomization list for each participating center. Batches of drug packages, each provided with a unique trial code, had been sent in advance to the participating general practices. A double-dummy technique achieved blinding of patients, treating physicians, and investigators to the assigned medication. This was necessary because amoxicillin and roxithromycin have different dosing schedules (3 times a day versus once daily) and are not identical in appearance (capsule versus tablet). All capsules and tablets had identical appearance and taste. All patients received both forms of their assigned medication. Compliance with medication regimens was measured by Medical Event Monitoring Systems (MEMS), an electronic recording system that compiles the dosing history of ambulatory patients taking oral medication.30
Chest X-Rays
Every patient underwent chest x-ray. The radiographs were reassessed for the presence or absence of infiltrate by a blinded independent senior radiologist. If the first and second radiologist disagreed, a third senior radiologist made a final assessment.
Follow-up
Follow-up consultations similar to the examination on day 1 took place on days 10 and 28. During treatment (days 1 through 10) and on days 21 and 27, follow-up was supplemented by a short diary in which patients recorded their symptoms and the times at which they resumed daily activities that they had abandoned or that had been impaired.
Outcomes measured
Efficacy was assessed by comparing the groups’ clinical response on day 10 (the primary outcome measure) and day 28 and their bacteriologic response on day 10. Satisfactory clinical response was defined in 4 ways: (1) decrease in symptoms of LRTI; (2) absence of symptoms of LRTI; (3) decrease in signs of LRTI; and (4) absence of signs of LRTI. All other outcomes were regarded as unsatisfactory responses.
Self-reported symptoms and time to resolution were compared between the 2 groups on days 1 through 10, 21, and 27. The percentage of patients who had abandoned daily activities or whose participation in daily activities had been impaired by illness was followed over time. Bacteriologic cure was defined as the absence of growth of a predominant bacterial pathogen (cultured at baseline) in a sputum sample taken on day 10.
We recorded patients’ compliance rates, frequency of adverse events, and acquired bacterial resistance. Compliance was defined as the number of doses taken divided by the number of doses prescribed.
Statistical analyses
The efficacy of amoxicillin and roxithromycin was evaluated using an intention-to-treat analysis. Differences were tested using a 2-sided chi-square test ( α= 0.05). Multiple logistic regression analysis was performed to analyze the effect of differences in baseline characteristics between the randomized groups. Differences in symptoms, time to resolution of symptoms, and time to resumption of abandoned and impaired daily activities were tested in life table analyses using the Gehan test. All statistical analyses were performed with Statistical Package for the Social Sciences software, version 8.0.
Results
Patient population
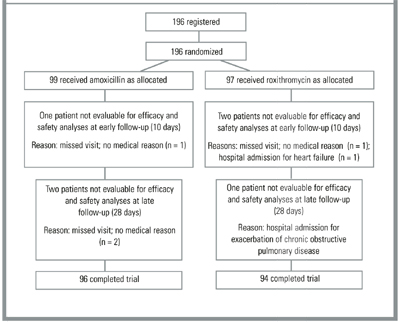
From January 1998 to April 1999, 25 PCPs from 15 practices recruited 196 patients aged 18 years to 89 years. Of these patients, 99 received amoxicillin and 97 received roxithromycin (Figure 1). The 2 groups’ demographic data, signs and symptoms, comorbidities, identified pathogens, and radiographic abnormalities were similar (Table 2). Multiple logistic regression analysis showed that none of the covariables altered the effects of the study medication.
TABLE 2
FINDINGS ON PRESENTATION
| Finding | Amoxicillin Group No. (%) | Roxithromycin Group No. (%) |
|---|---|---|
| Number of Patients | 99 (51) | 97 (49) |
| Demographic Data | ||
| Ratio of men to women | 46/53 | 53/44 |
| Mean age in years (SD) | 55 (15) | 50 (16) |
| Symptoms | ||
| Recent cough in number of days | ||
| 1–7 | 34 (36) | 41 (43) |
| 8–14 | 31 (33) | 25 (26) |
| 15–28 | 22 (23) | 23 (24) |
| No recent cough | 8 (8) | 6 (6) |
| Productive cough | 77 (78) | 84 (88) |
| Dyspnea | 78 (79) | 76 (79) |
| Wheezing | 68 (69) | 61 (64) |
| Risk Factors | ||
| Cigarette smoking | 36 (36) | 29 (31) |
| Comorbidity | ||
| None | 55 (56) | 48 (52) |
| Asthma | 19 (19) | 20 (22) |
| COPD | 17 (17) | 11 (12) |
| Heart failure | 3 (3) | 4 (4) |
| Diabetes mellitus | 2 (2) | 3 (3) |
| Other | 23 (24) | 21 (23) |
| Asthma medication prescribed at start of study | 16 (16) | 13 (14) |
| Signs | ||
| Auscultation abnormalities | 93 (94) | 87 (91) |
| Body temperature 38.0°C | 25 (26) | 22 (24) |
| Infection | ||
| Mild/moderate | 91 (93) | 89 (93) |
| Severe | 7 (7) | 7 (7) |
| Laboratory Tests | ||
| CRP, median (range) | 23 (2-228) | 26 (2-312) |
| ESR, median (range) | 21 (1-104) | 19 (1-121) |
| Leukocytes, median (range) | 8.3 (3.9-19.7) | 8.4 (4.3-15.4) |
| Patients with pathogens | 45 (45) | 46 (47) |
| Chest X-Ray | ||
| Infiltrate on chest x-ray | 14 (14) | 13 (14) |
| NOTE: Values are numbers (percentages) unless otherwise stated. Percentages are based on number of patients for each variable. | ||
| COPD denotes chronic obstructive pulmonary disease; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; SD, standard deviation. | ||
FIGURE 1
DISTRIBUTION OF PATIENTS FOR EFFICACY AND SAFETY ANALYSES
Clinical cure
Early Follow-Up. The rate of clinical cure, defined as the decrease in symptoms and signs at 10 days after randomization, was high and not significantly different between both groups. Using the stricter definition of clinical cure as the complete absence of symptoms and signs led to the same conclusion. Absolute cure rates using this strict definition were low (Table 3).