Physicians discontinued treatment with the study medication in 2 cases (1 amoxicillin and 1 roxithromycin) because of unsatisfactory clinical response. Both patients recovered rapidly after alternative antibiotic treatment. In one case, the patient discontinued amoxicillin after 8 days because of rash and urticaria and recovered quickly without further treatment.
Late Follow-Up. According to the physicians’ final assessments, the rate of clinical cure at 28 days was not significantly different between the 2 groups, although the percentage of patients who showed a decrease in symptoms was significantly higher in the amoxicillin group than in the roxithromycin group (Table 3). Again, cure rates were much lower when the strict definition of cure was used. Eleven patients in the amoxicillin group and 8 in the roxithromycin group were not clinically cured after 28 days. Of these patients, 10 (5 in each group) recovered shortly thereafter or did not consult their physician again for persisting symptoms of LRTI. Nine patients (6 in the amoxicillin group, 3 in the roxithromycin group) with exacerbation of COPD slowly returned to their baseline clinical situation. Four patients (3 in the amoxicillin group, 1 in the roxithromycin group) were found to have concomitant pulmonary cancer. Curative bilobectomy was performed in one of the patients. The others received palliative treatment.
TABLE 3
CLINICAL CURE RATE AT EARLY (10-DAY) AND LATE (28-DAY) FOLLOW-UP
| Characteristic | Amoxicillin No. (%) | Roxithromycin No. (%) | Relative Risk* (CI) |
|---|---|---|---|
| Decrease in Symptoms and Signs | |||
| Day 10 | |||
| Symptoms | 84/96 (88) | 90/95 (95) | 2.38 (0.87-6.48) |
| Signs (physical examination) | 85/98 (87) | 89/95 (94) | 2.10 (0.83-5.30) |
| Day 28 | |||
| Symptoms | 91/95 (96) | 79/93 (85) | 0.28 (0.10-0.82)† |
| Signs (physical examination) | 90/96 (94) | 87/94 (93) | 0.74 (0.29-2.41) |
| Absence of Symptoms and Signs | |||
| Day 10 | |||
| Symptoms | 18/96 (19) | 22/95 (23) | 2.38 (0.87-6.48) |
| Signs (physical examination) | 68/98 (69) | 76/95 (80) | 1.53 (0.93-2.53) |
| Day 28 | |||
| Symptoms | 59/95 (62) | 50/93 (54) | 0.82 (0.58-1.15) |
| Signs (physical examination) | 82/96 (85) | 80/94 (85) | 0.98 (0.49-1.94) |
| Fever (≥38°C) gone, day 10 | 21/25 (84) | 16/22 (73) | 1.37 (0.25-7.41) |
| Cure, final conclusion by physician, day 28 | 84/95 (88) | 86/94 (91) | 1.36 (0.57-3.23) |
| NOTE: Percentages are based on number of patients for each variable. | |||
| *Risk of no cure with amoxicillin vs roxithromycin. | |||
| †P < .05. | |||
Self-reported response over time
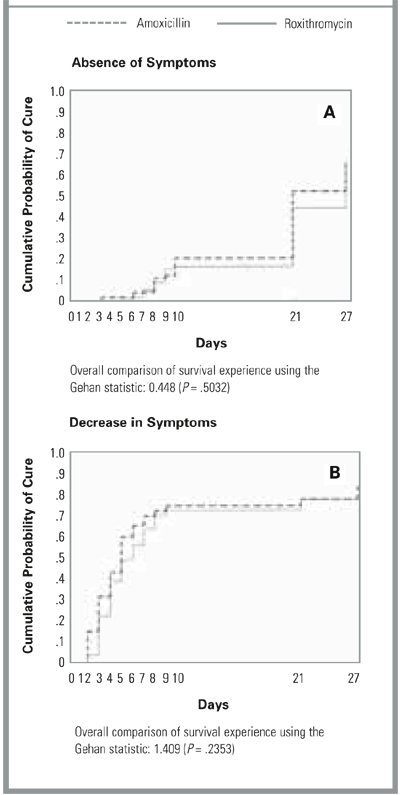
The time before resolution of symptoms according to the patients’ diaries was similar for patients treated with amoxicillin and those treated with roxithromycin (Figures 2A and 2B). The percentage of patients who had abandoned daily activities was followed over time. At baseline, more than half of the patients in the amoxicillin group and fewer than 40% in the roxithromycin group reported that they had abandoned daily activities. At day 10, this percentage had fallen to less than 20% in both groups and to less than 10% in both groups at day 28. Differences between the amoxicillin and roxithromycin groups were not significant.
Furthermore, the patients’ diaries revealed information about the time of impaired daily activities. The percentage of patients with impaired daily activities gradually decreased in both treatment groups from approximately 75% at baseline to 30% at day 10 and 20% at day 28.
FIGURE 2
TIME TO RESOLUTION OF SYMPTOMS AS DESCRIBED IN PATIENTS’ DIARIES
Subgroup analyses
The above analyses were repeated for a group of patients aged less than 65 years and a group aged 65 years and older. The trend in cure rates was the same. No differences were found between these age groups regarding the percentage of patients with satisfactory clinical response. Furthermore, the same analyses were performed for each of the clinical diagnoses made by the PCPs at baseline (ie, pneumonia, acute bronchitis, exacerbation of asthma or COPD, and unclassified LRTI). Overall, no significant differences were found between the amoxicillin and roxithromycin groups.
Bacteriologic evaluation
Pathogens were identified in 91 patients (46%). Viruses were most frequent, followed by H (Para) influenzae, S pneumoniae, and Moraxella catarrhalis (Table 4). Bacteriologic cure was achieved in 21 of the 23 patients (91%) in the amoxicillin group and in 23 of the 27 patients (85%) in the roxithromycin group (NS, Fisher’s exact test). In 9 patients of the amoxicillin group and 8 patients of the roxithromycin group, only the sample obtained after 10 days showed the growth of a predominant bacterial pathogen (superinfection).
TABLE 4
RESPIRATORY TRACT PATHOGENS ISOLATED
| Microorganism | No. (%) |
|---|---|
| Typical Bacterial Pathogens | |
| Haemophilus (Para) influenzae | 34 (17) |
| Streptococcus pneumoniae | 12 (6) |
| Moraxella catarrhalis | 6 (3) |
| Other* | 5 (3) |
| Atypical Pathogens | |
| Mycoplasma pneumoniae | 2 (1) |
| Legionella pneumophila | 1 (0.5) |
| Viruses | |
| Influenza A | 29 (16) |
| Influenza B | 7 (4) |
| Parainfluenzae 1, 2, 3 | 7 (4) |
| Adenovirus | 5 (3) |
| Respiratory syncytial virus | 5 (3) |
| No organism (number of patients) | 122 (49) |
| * Enterobacteriaceae (n = 2), Staphylococcus aureus (n = 1), Streptococcus viridans (n = 1), Neisseria meningitidis (n = 1). | |
Safety and compliance
Thirty possible or probable adverse events were reported in 19 of 99 patients (19%) treated with amoxicillin: diarrhea (13), stomach ache (3), headache (3), and 11 other side effects, including nausea, vomiting, and rash, once each. In the roxithromycin group, 24 events were reported in 16 patients (16%): nausea (5), diarrhea (4), vomiting (4), rash (2), headache (2), and 7 others, including pruritus ani, dizziness, and mild bradycardia, once each.