Your patient comes in complaining of acute eye pain. Is it an ophthalmic emergency? Benign? Something in between?
The varying degrees of severity are reflected in the cases presented here, and in the multiple-choice quiz that follows. After selecting your answer to each of the questions, turn the page to find out if you were right.
CASE 1 A 74-year-old man presents with left eye pain that began when he lowered the shades in his bedroom to get ready for a nap. The pain worsened rapidly, he reports, and now—a half hour later—he has a headache, nausea, and blurred vision in the affected eye.
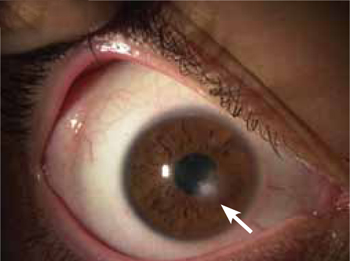
The patient has a history of hypertension, which is controlled with hydrochlorothiazide, but takes no other drugs. He denies any eye trauma. An eye exam reveals that the pupil is dilated and reacts poorly to light; you note corneal haziness and edema, as well ( FIGURE 1; vertical line is the slit lamp beam).
FIGURE 1

What’s your diagnosis?
- angle-closure glaucoma
- macular degeneration
- open-angle glaucoma
- retinal detachment.
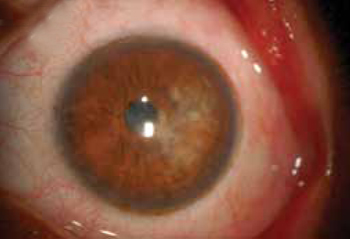
CASE 2 A 20-year-old man was playing touch football while wearing contact lenses. Soon after, the game, he felt a stinging sensation in his right eye—”like sand under the eyelid,” he said. Exposure to sunlight also produced eye pain. The patient had tried flushing his eye with water, but experienced little pain relief.
An eye exam reveals a grayish-white spot in the line of vision ( FIGURE 2 ), with no sign of a penetrating injury.
FIGURE 2
What’s your next step?
- Prescribe antibiotic eye drops and send the patient home.
- Provide an emergent ophthalmology referral for foreign body extraction.
- Send the patient home with an eye patch to relieve the photophobia.
- Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
CASE 3 A 17-year-old woman is brought in by her mother because of pain and vision loss in her right eye. The pain started as soon as she awoke; 2 hours later, the vision in the affected eye became blurry. Soon after, she saw spots of light, followed by complete loss of vision. She denies any trauma and says she has never experienced anything like this before.
The patient’s visual acuity is 20/200 in her right eye, and 20/40 in the left. You follow up with a funduscopic exam of the eye, which shows edema of the optic disc, blurring of the disc margins, and distended veins ( FIGURE 3 ).
FIGURE 3

What diagnostic test should be next?
- fluorescein angiography
- intraocular pressure measurement
- magnetic resonance imaging (MRI) of the brain
- visual fields assessment.
CASE 4 A 31-year-old woman with a history of sarcoidosis comes in because of spontaneous redness ( FIGURE 4 ) and pain in her left eye, which began early that day. She denies any eye trauma, eye surgery, or recent cold, and has no discharge or crust around the eye.
FIGURE 4

What’s your diagnosis?
- anterior uveitis
- conjunctivitis
- corneal abrasion
- posterior uveitis.
CASE 5 A 21-year-old college student complains of pain in her left eye that started a day ago. She wears contact lenses and, upon questioning, tells you that she sometimes keeps them in all night.
The patient reports that she used a friend’s steroid eye drops twice yesterday, but the drops didn’t help. The pain is worse today. It feels as if there’s something in her eye, she says, and she finds it hard to open her eye. Penlight examination ( FIGURE 5 ) reveals a branching opacity on the cornea.
FIGURE 5
What’s your next step?
- Advise the patient to stop wearing her contact lenses overnight, give her a cycloplegic, and follow up in 2 days.
- Patch the patient’s left eye, prescribe antibiotics, and tell her to return tomorrow.
- Prescribe steroid eye drops and follow up in 2 days.
- Provide an urgent referral to an ophthalmologist.
CASE 1 The answer is A: angle-closure glaucoma.
Glaucoma is the world’s leading cause of blindness,1,2 and angle-closure glaucoma comprises 10% of cases.2 In this condition, the anterior chamber angle—formed by the iris and the cornea—is narrow. When the iris dilates in low light (eg, the darkened room in which the patient had planned to nap), it folds into the narrowed angle, preventing the flow of aqueous humor and leading to an increase in intraocular pressure.3