A systematic approach to postdelivery evaluation
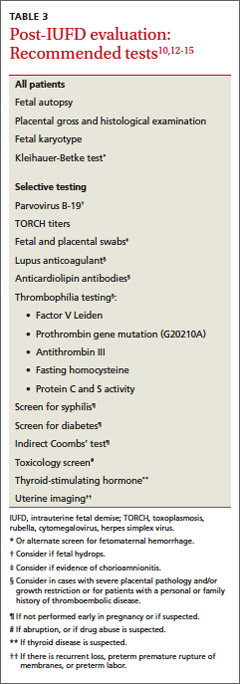
Although 25% to 60% of IUFDs are classified as “unexplained,” in up to 40% of cases the lack of explanation may be due to an incomplete evaluation.2-4 When performing an evaluation, it is important to be systematic and not confuse association with causality. Kortweg et al13 analyzed laboratory studies obtained in the evaluation of 1025 fetal deaths in the Netherlands from 2002 to 2008. The most useful tests were placental examination, fetal autopsy, and fetal karyotype, which aided in assigning the cause of death in 96%, 73%, and 29% of cases, respectively. Compared to fetal karyotyping from postpartum tissue sampling, samples obtained via amniocentesis or chorionic villus sampling before inducing labor are much more successful in identifying the cause of death (85% vs 28%).14
Testing for fetomaternal hemorrhage, which is the cause of IUFD about 12% of the time, needs to be performed when IUFD is diagnosed.13 Additional laboratory testing may be helpful depending on the mother’s history or symptoms at the time of IUFD. For example, a maternal history of drug use, thyroid disease, diabetes mellitus, hypertension, venous thromboembolism, or febrile illness should prompt further studies (TABLE 3).10,12-15
How to help grieving parents
Mothers may feel tremendous guilt upon suffering an IUFD. When addressing grief, mourning, and bereavement after an IUFD, the goal is to support the parents through the grieving process and properly identify when grief becomes pathologic. Grief is pathologic when there is a prolonged response—usually longer than 6 months—and when it interferes with daily activities.16 In a prospective study, patient characteristics that affected the intensity of grief were advanced gestational age at loss, lack of children in the home, relatively older age, pre-loss neurotic personality, and pre-loss psychiatric symptoms.17
Unlike the grief experienced by parents who lose an infant or child, the grief experienced by parents who experience an IUFD may not be socially validated. Therefore, it is important for physicians to acknowledge that patients’ feelings of loss are legitimate. Additionally, reassure mothers that there was very likely nothing that she could have done to change the outcome, unless there is compelling evidence to the contrary (eg, drug abuse causing abruption and fetal demise). Avoid using phrases such as “you can always try again.”
In a study of 769 women who experienced an IUFD, many reported receiving “support” or “great support” from family members (91.7%), nurses (90%), and physicians (53.4%).18 Adequate health care support is associated with lower levels of depression and anxiety, but family support appears to be the most important.18 Women who are single, divorced, or widowed experience higher levels of depression after IUFD than those who are married or cohabitating.18
In a different study of support for women who experienced IUFD or death of their child shortly after birth, mothers did not blame doctors or feel that the doctors should make them feel better.19 However, they did want an explanation in simple language of what had gone wrong and for physicians to listen and accept their distress.19 This study also found that early support and counseling shortened the bereavement process.19 Half of women had symptoms of depression and anxiety 6 months after the death of their fetus or child and 20% had these symptoms at 14 months. Fathers, however, recovered more quickly—14% were symptomatic at 6 months.19
Managing a subsequent therapy
A retrospective cohort study found that for women who had experienced an IUFD, the odds ratio of having a recurrent IUFD was 1.94 (99% confidence interval, 1.29-2.92) compared to women who had a previous live birth.20 The risk of recurrent IUFD in a specific patient is related to the underlying pathophysiologic cause of the initial IUFD, and how that cause was addressed. For example, a patient who experienced an IUFD believed to be the result of uncontrolled diabetes can expect to have an improved outcome if her diabetes is brought under control before conceiving and she maintains control throughout the pregnancy. On the contrary, a patient who experienced an IUFD that was believed to be secondary to a nonmodifiable risk factor, such as lupus-induced chronic kidney disease, will continue to have a significant risk of recurrence of IUFD in the subsequent pregnancy.
When managing a subsequent pregnancy of a woman who has experienced an IUFD, review all data from the prior pregnancy as well as the mother’s medical conditions. Order any studies in TABLE 3 that were not previously obtained and are clinically indicated. If applicable, encourage the woman to quite smoking and achieve a healthy BMI (<25).