SAN DIEGO – Children who parents describe as “always sick” often are immunologically normal, but knowing when to suspect otherwise is crucial, according to Dr. Meg Fisher.
“When parents tell you their child is sick all the time, they are. They’re literally just recovering from one thing when they pick up the next,” said Dr. Fisher, a pediatric infectious diseases specialist at Monmouth Medical Center in West Orange, N.J.
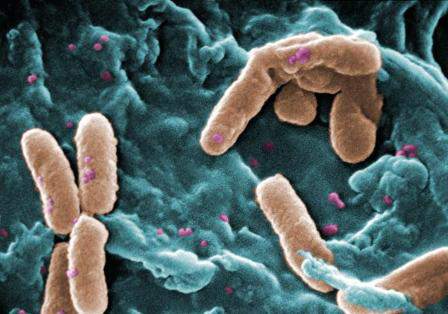 CDC/Janice Haney Carr
CDC/Janice Haney Carr
Pseudomonas is often isolated from stool samples, but is not normally found in a child’s respiratory tract.
Children under 2 years of age typically acquire 4-10 symptomatic respiratory infections per year – and up to 13 if they are in day care, Dr. Fisher said. These children also normally develop one to four gastrointestinal infections per year, she added. And children older than 2 years average four to eight respiratory infections and up to two gastrointestinal infections annually, she said at the annual meeting of the American Academy of Pediatrics .
Certain types of infections always merit a closer look, Dr. Fisher emphasized. Invasive infections, recurrent meningitis, excessive episodes of respiratory disease, chronic diarrhea, recurrent urinary tract infections, and recurrent skin and soft tissue infections can indicate immunodeficient disorders, inherited diseases such as cystic fibrosis, or anatomic abnormalities that predispose children to serious infections, she said. “The site of recurrent infections is really going to help you determine which subspecialist you need,” she added.
Culture results also provide clues about underlying conditions. “If you ever recover Pseudomonas aeruginosa from the respiratory tract of a child, you should automatically think about cystic fibrosis,” Dr. Fisher said. Pseudomonas is often isolated from stool samples, but is not normally found in a child’s respiratory tract, she explained.
“Unusual organisms and abnormal laboratory results should always trigger a follow-up evaluation,” Dr. Stuart Abramson said in a related presentation. The most common primary immunodeficiency disorders include selective IgA deficiency – which affects 1 in 500 children – IgG2deficiency, transient hypogammaglobulinemia of infancy, and DiGeorge anomaly, said Dr. Abramson, who is director of allergy and immunology services at Shannon Medical Center in San Angelo, Tex. Less common primary immunodeficiencies affect 1 in 50,000 to 1 in 200,000 children and include B-cell disorders, T-cell disorders, phagocytic disorders, and complement disorders, he said at the meeting.
Of the four stages of testing for primary immunodeficiencies, only the first stage needs to be done by the primary care pediatrician; testing at the first stage includes taking a history and physical examination, complete blood count and differential, and quantitative immunoglobulin levels for IgA, IgG, and IgM, said Dr. Fisher. A child who needs further testing “might be better served by an immunologist,” she added.
Pediatricians should consider first-stage testing if a patient presents with one or more warning signs of a primary immunodeficiency in children, Dr. Abramson said.
Those warning signs are:
• Four or more new ear infections within 1 year.
• Two or more serious sinus infections within 1 year.
• Two or more months on antibiotics with little effect.
• Two or more pneumonias within 1 year.
• Failure of an infant to gain weight or grow normally.
• Recurrent, deep abscesses of the skin or organs.
• Persistent oral thrush or cutaneous mycoses.
• Need for intravenous antibiotics to clear infections.
• Two or more deep-seated infections, including septicemia.
• A family history of primary immunodeficiency.
(This list was assembled by the Jeffrey Modell Foundation.)
Dr. Fisher and Dr. Abramson declared no relevant financial relationships.