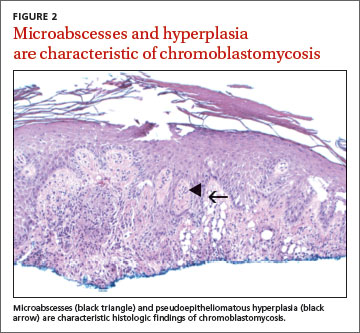
The punch biopsy revealed pseudoepitheliomatous hyperplasia with intraepidermal microabscesses (FIGURE 2), which was consistent with chromoblastomycosis. Two additional biopsies taken from plaques on the patient’s arm grew Phialophora verrucosa, confirming the diagnosis. We assumed she contracted chromoblastomycosis from her exposure to the overseas crates at her job, but we could not confirm this. However, there were no other likely sources of infection.
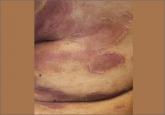
Chromoblastomycosis is a subcutaneous fungal infection that is endemic to tropical and subtropical climates but sporadically occurs elsewhere. It is caused by inoculation from soil contaminants. The characteristic plaques begin as small pink papules and may slowly progress to thick verrucous and somewhat scaly plaques or nodules.1 The plaques usually first appear on the lower legs and feet, but may occur on the upper limbs and trunk. They typically progress locally, although they may spread to distant areas, including the face, by self-inoculation. These plaques may cause minimal symptoms or significant morbidity, including lymphedema and elephantiasis.1,2