Keith R. Campbell, PharmD, MBA, CDE Distinguished Professor in Diabetes Care and Pharmacotherapy, Department of Pharmacotherapy, Washington State University College of Pharmacy, Pullman, Washington
Michael E. Cobble, MD, FNLA Director, Canyons Medical Center, Sandy, Utah, Adjunct Faculty, University of Utah School of Medicine, Salt Lake City, Utah
Timothy S. Reid, MD Department of Family Medicine, Mercy Diabetes Center, Janesville, Wisconsin
Mansur E. Shomali, MD, CM Clinical Associate Professor of Medicine, University of Maryland School of Medicine, Associate Medical Director, Diabetes and Endocrine Center, Union Memorial Hospital, Baltimore, Maryland
References
The reason for the difference between GLP-1 agonists and DPP-4 inhibitors with respect to weight remains unclear, but may result from the direct action of GLP-1 agonists on the GLP-1 receptor compared to the indirect action of DPP-4 inhibitors, which slow the clearance of endogenous GLP-1.25 This may explain the ability of GLP-1 agonists—but not DPP-4 inhibitors—to promote satiety and reduce caloric intake.26,27 In a crossover comparison of exenatide with sitagliptin, caloric intake during a standardized meal decreased with exenatide (–134 kcal) and increased with sitagliptin (+130 kcal) (P=.0227).16
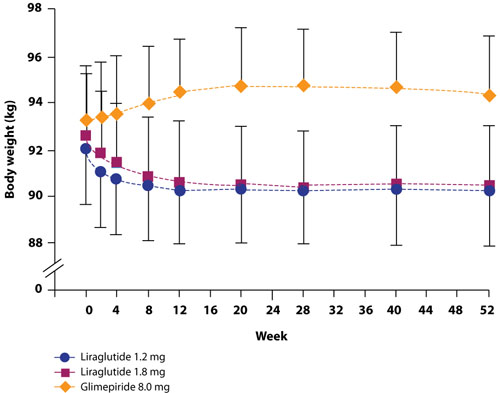
The possibility that the nausea associated with GLP-1 agonists but not DPP-4 inhibitors is the reason for the difference in weight effects has been investigated. Analyses have shown, however, that the weight loss observed with GLP-1 agonists is independent of nausea.4,10,28 For example, in a study by Garber et al,4 there was no difference in the amount of weight lost among patients who experienced liraglutide-associated nausea for >7 days, for 1 to 7 days, or not at all. The finding that nausea generally resolved within the first few weeks of liraglutide treatment, while weight loss was maintained over the 52 weeks of the trial, provides further evidence that nausea is not the cause of weight loss (FIGURE 1).4 Similar long-term weight loss has been observed with exenatide: weight loss was achieved through 30 weeks (–3.0 kg; P<.05 vs baseline) of double-blind treatment and maintained during an additional 52 weeks of open-label treatment (–5.3 kg; P<.05 vs baseline).29
FIGURE 1Change in body weight (kg) over 52 weeks with liraglutide 1.2 mg and 1.8 mg vs glimepiride 8.0 mg4
Garber A, Henry R, Ratner R, et al. Liraglutide versus glimepiride monotherapy for type 2 diabetes (LEAD-3 Mono): a randomised, 52-week, phase III, double-blind, parallel-treatment trial. Lancet, 2009;373:473-481. Reprinted with permission. Copyright Elsevier, 2009.
cardiovascular benefits
The effects of incretin therapy on markers of cardiovascular disease have been assessed in several clinical trials (TABLE 1).4,8-12,17,22,30,31 In general, these trials demonstrate small but significant reductions in systolic blood pressure (1 to 7 mm Hg) with the GLP-1 agonists; diastolic blood pressure, however, is not significantly affected.4,8-12,30,31 There are insufficient data regarding the DPP-4 inhibitors.17,22
Effects on the lipid profile also have been investigated,4,5,8-12,17,22,30,31 but differences among the agents are difficult to assess because of different baseline lipid levels and the limited number of direct comparative studies. In general, clinical studies show that low-density lipoprotein (LDL) cholesterol is reduced by 1 to 17 mg/dL with the GLP-1 agonists and increased by 3 to 9 mg/dL with the DPP-4 inhibitors. Changes in high-density lipoprotein (HDL) cholesterol are generally small for both GLP-1 agonists and DPP-4 inhibitors, ranging from an increase of 5 mg/dL to a decrease of 2 mg/dL. The greatest change in the lipid profile is in the triglyceride level, with a reduction of 12 to 40 mg/dL with the GLP-1 agonists, while the triglyceride changes observed with the DPP-4 inhibitors range from a reduction of 35 mg/dL to an increase of 16 mg/dL.
Two studies have directly compared the effects on the lipid profile of 2 incretin agents over 26 weeks. In the first study, exenatide and liraglutide showed similar changes in LDL cholesterol (–7 vs –8 mg/dL, respectively) and HDL cholesterol (–1 vs –1 mg/dL, respectively) levels, but liraglutide showed a significantly greater reduction in triglyceride levels than exenatide (–36 vs –20 mg/dL, respectively; P=.0485).12 The second study compared liraglutide 1.2 mg and 1.8 mg once daily and sitagliptin 100 mg once daily.5 LDL cholesterol increased by 1 mg/dL in both liraglutide groups and by 2 mg/dL in the sitagliptin group, while there was no change in HDL cholesterol with either dose of liraglutide or sitagliptin. The triglyceride level decreased by 17 mg/dL in the liraglutide 1.2 mg group, 38 mg/dL in the liraglutide 1.8 mg group, and 35 mg/dL in the sitagliptin group. None of the differences between either liraglutide group and sitagliptin were statistically significant.
Effects on the lipid profile appear to be durable. Klonoff et al showed that the effects of exenatide on the lipid profile were sustained over 3.5 years of follow-up (in a 30-week randomized, double-blind trial followed by a 3-year open-label extension).14 In patients younger than 65 years, changes from baseline were as follows: total cholesterol, –10 mg/dL (P=.0056); LDL cholesterol, –11 mg/dL (P=.0012); HDL cholesterol, +8 mg/dL (P<.0001); and triglycerides, –44 mg/dL (P=.0042). Similar changes were observed in those 65 years and older.
The cardiovascular benefits of incretin therapy may extend beyond blood pressure and the lipid profile. An exploratory subanalysis of a randomized controlled trial with liraglutide showed a significant decrease in plasminogen activator inhibitor-1, an inflammatory biomarker, and B-type natriuretic peptide, a marker of left ventricular dysfunction.32 No significant effect on high-sensitivity C-reactive protein, interleukin-6, or tumor necrosis factor-α was observed.