The most predictive finding for osteoarthritis is decreased range of motion with restriction in internal rotation (LOE=1b).12 For those patients with one plane of restricted movement, the sensitivity for osteoarthritis is 100% and specificity is 42%; in 3 planes of restricted movement, sensitivity is 54% and specificity is 88% with a likelihood ratio of 4.4.12 A positive FABER test has been shown to be 88% sensitive for intra-articular pathology in an athletic population.16
Muscle testing. Test muscle strength to assess whether particular muscle groups are the source of pain. Maneuvers include resisted hip flexion, adduction, abduction, external rotation, and extension.
Other tests. With lateral hip pain, findings of weakness or pain while testing hip abduction may point to gluteus medius muscle dysfunction associated with greater trochanteric pain syndrome. The Trendelenburg test may also help. The patient stands on the affected leg. A negative test result occurs when the pelvis rises on the opposite side. A positive test result occurs when the pelvis on the opposite side drops and indicates a weak or painful gluteus medius muscle.
With Ober's test, the patient lies on his or her side with hips and knees flexed. The upper leg is passively extended then lowered to the table. Lateral hip pain or considerable tightness may indicate iliotibial band syndrome.
With the Thomas test, the contralateral hip is flexed, and the symptomatic hip is moved from full flexion to full extension. A deep click palpated may be indicative of a labral tear.
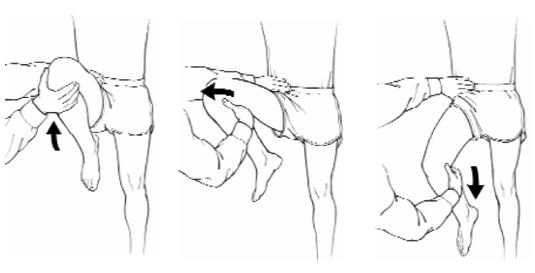
The snapping hip maneuver (Figure 6) may also be helpful in diagnosing the cause of pain. Loss of sensation to the anterolateral thigh is consistent with meralgia paresthetica.
Palpation. Finally, palpate over specific structures, such as the hip flexor muscles, greater trochanter, iliotibial band, and gluteus medius muscle, to further localize the source of pain. For instance, tenderness may be present over the anterior soft tissues in a hip flexor muscle strain or iliopsoas bursitis, and over the greater trochanter in trochanteric bursitis.
FIGURE 5
FABER test
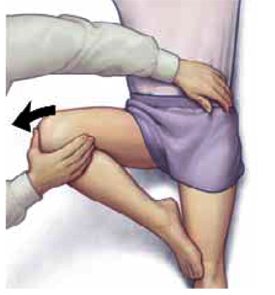
FIGURE 6
Snapping hip maneuver
When diagnostic imaging is beneficial
In most cases, a thorough history and physical examination are adequate to establish a diagnosis. In the Lamberts study,5 only 16% of hip complaints required imaging for further elucidation. (Table 2) summarizes use of imaging studies with different disorders.
X-ray studies
Patients with a history of traumatic injury, osteoporosis, cancer, high-dose corticosteroid exposure, or alcohol abuse are at higher risk of such bony hip pathology as fracture, osteoarthritis, or avascular necrosis. These patients should undergo x-ray studies during their initial evaluation. An anteroposterior pelvic radiograph and a lateral radiograph of the hip are appropriate.
Although no specific patient age has been identified as a threshold for ordering x-ray studies, we recommend that all patients older than 65 years with new-onset hip pain undergo such studies.
We also recommend x-ray films for a patient of any age who has chronic severe hip pain.
TABLE 2
Indications for diagnostic imaging studies
| Disorder | Test | Level of evidence |
|---|---|---|
| Osteoarthritis | AP and lateral hip x-ray studies—weight-bearing17 | 2 |
| Muscle strain/tendonitis | None needed initially; consider MRI if not resolving | 5 |
| Greater trochanteric pain syndrome | None needed initially; consider MRI if not resolving9 | 4 |
| Hip fracture (proximal femur) | AP pelvis and cross table lateral x-ray studies | * |
| Stress fracture | MRI—sensitivity 100%13 | 4 |
| Iliopsoas bursitis | None needed initially; consider MRI if not resolving Can also use iliopsoas bursa imaging18-20 | 4 |
| Iliotibial band syndrome | None needed initially; consider MRI if not resolving | 5 |
| Meralgia paresthetica | Usually diagnosed by history. Can use sensory nerve conduction study21 | 4 |
| Inflammatory arthritis | Complete blood count, erythrocyte sedimentation rate or C-reactive protein, arthrocentesis, x-ray study | * |
| Referred pain from lumbar spine | MRI of lumbar spine | * |
| Avascular necrosis of femoral head | AP and lateral hip x-rays MRI for staging22 | 4 |
| Acetabular labral tear | MR arthrography—sensitivity 91%, specificity 71%23 25 | 4 |
| *Level of evidence not reported as specific references could not be found. | ||
| AP, anteroposterior; MRI, magnetic resonance imaging | ||
Magnetic resonance imaging
Advanced imaging may be required when initial conservative therapy is not effective or x-ray findings are unrevealing. Although computed tomography (CT) scan and bone scan have roles in the evaluation of some hip disorders, MRI has emerged as the study of choice in diagnosing hip pathology, especially in athletes.13
MRI offers valuable information regarding occult bony and cartilage injury such as stress fractures, avascular necrosis, and osteoarthritis, as well as soft tissue abnormalities such as muscle tears and bursitis. In a retrospective study of patients with suspected hip fracture but negative plain film results, MRI showed occult femoral fractures in 37% of patients, occult pelvic fractures in 23%, and associated soft-tissue abnormalities such as muscle edema and hematoma or joint effusion in 74%.26
Other imaging tests